

Time to revisit the problem of CIN? The low incidence of acute kidney injury with and without contrast in hospitalized patients: an observational cohort study
- PMID: 26462259
- PMCID: PMC4601139
- DOI: 10.1186/s40697-015-0073-6
Time to revisit the problem of CIN? The low incidence of acute kidney injury with and without contrast in hospitalized patients: an observational cohort study
Abstract
Background: Acute kidney injury (AKI) following imaging procedures with contrast medium in hospitalized patients is commonly attributed to contrast-induced nephropathy (CIN). This study sought to establish a benchmark of the incidence of AKI in hospitalized patients who underwent computed tomography (CT) scans, with and without intravenous contrast administration.
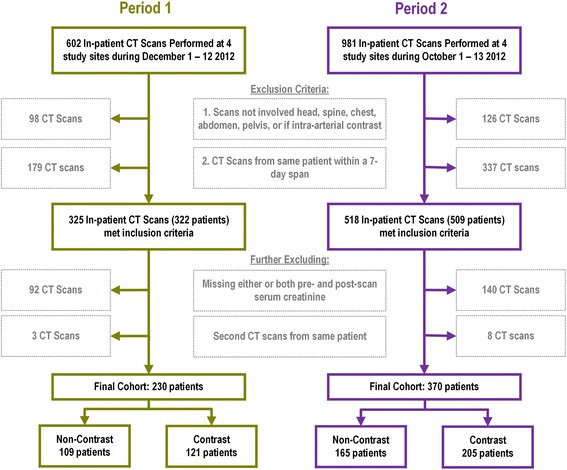
Methods: This was a multi-center observational cohort study. Hospitalized patients in four hospitals with CT scans during two time periods in 2012 and 2013 were included. AKI post-scan was defined as a change in serum creatinine (sCr) in absolute terms of ≥26.5 μmol/L (≥0.3 mg/dl), occurring within 7 days of the CT scan. AKI incidence was examined by study phases and CT-scan types using logistic regression models. Multinomial logistic regression was used to examine the proportions of sCr availability between two study phases.
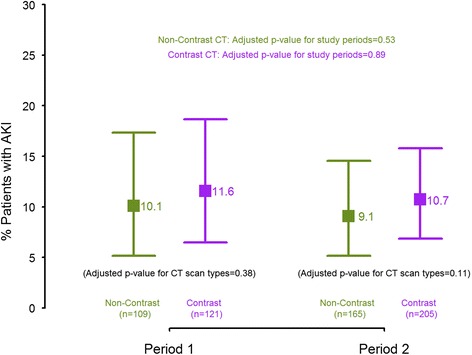
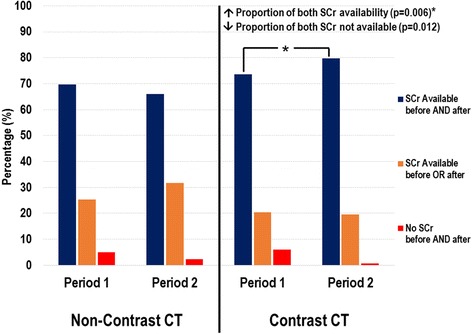
Results: Three hundred and twenty-five patients in Period 1 and 518 patients in Period 2 were included in the study. The incidence of AKI in Period 1 was similar in those who received contrast and in those who did not (11.6 % [95 % C.I.: 6.5, 18.7] vs. 10.1 % [95 % C.I.: 5.1, 17.3]; p = 0.38). The incidence of AKI remained not significantly different between the two periods in those who received contrast (11.6 % [95 % C.I.: 6.5, 18.7] vs. 10.7 % [95 % C.I.: 6.8, 15.8]; p = 0.89) and those who did not (10.1 % [95 % C.I.: 5.1, 17.3] vs. 9.1 % [95 % C.I.: 5.2, 14.6]; p = 0.54). Among those who received contrast, there was a significant increase in the availability of both pre- and post- CT scan sCr in Period 2 compared to Period 1 (73.6 % [95 % C.I.: 67.7, 80.6] vs. 79.8 % [95 % C.I.: 75.2, 84.7]; p = 0.006).
Limitations: Our study was not targeted to specifically assess the impact of a prevention protocol on the incidence of AKI and was limited to settings within one health authority in the province.
Conclusion: In hospitalized patients, the incidence of AKI is low, not different between those who did and did not receive contrast, and was not impacted by improvement in the monitoring of sCr in at risk patients. A better understanding of the determinants of AKI post-contrast scan is required to improve strategies to reduce the incidence of AKI.
Données connues: L’occurrence d’un épisode d’insuffisance rénale aiguë (IRA) à la suite d’examens d’imagerie médicale avec administration d’un agent de contraste est fréquemment attribuée à une néphropathie induite par l’agent de contraste lui-même. La présente étude a cherché à établir des bases de référence susceptibles d’aider à mesurer l’incidence des épisodes d’IRA chez les patients hospitalisés qui ont à subir un examen par tomodensitométrie (scanner), avec ou sans administration intraveineuse d’un agent de contraste.
Méthodologie: Cette étude observationnelle a été réalisée sur des cohortes de patients hospitalisés sélectionnés dans les unités de néphrologie de quatre centres hospitaliers différents. Ces patients ont subi des examens par tomodensitométrie au cours de deux périodes distinctes en 2012 et en 2013. Il a été décrété que les patients étaient atteints de néphropathie post-scanner lorsque leur taux de créatinine sérique augmentait de plus de 26.5 μmol/L ou à 0.3 mg/dl dans les 7 jours suivant l’examen. L’incidence d’insuffisance rénale aiguë a été analysée à l’aide d’un modèle de régression logistique en fonction de la phase de l’étude et du type de tomodensitomètre utilisé pour l’examen. Une régression logistique multinomiale a été utilisée pour présenter les taux de créatinine sérique mesurés entre les phases de l’étude.
Résultats: La cohorte de la phase 1 comptait 325 patients et celle de la phase 2 en comptait 518. Il en est ressorti que l’incidence d’IRA post-scanner était similaire chez tous les patients de la phase 1, qu’ils aient ou non reçu un agent de contraste par intraveineuse avant l’examen (11.6 % [95 % I.C: 6.5, 18.7] vs 10.1 % [95 % I.C: 5.1, 17.3]; p = 0.38). L’incidence des épisodes d’IRA post-scanner est demeurée similaire dans les deux phases pour les patients ayant reçu un agent de contraste (11.6 % [95 % I.C: 6.5, 18.7] vs 10.7 % [95 % I.C: 6.8, 15.8]; p = 0.89) de même pour les patients n’en ayant pas reçu (10.1 % [95 % I.C: 5.1, 17.3] vs 9.1 % [95 % I.C: 5.2, 14.6]; p = 0.54). Chez les sujets ayant reçu un produit de contraste, il y avait une plus grande disponibilité des mesures de créatinine sérique pré — et post-scanner dans la période 2 par rapport à la période 1 (73.6 % [95 % I.C: 67.7, 80.6] vs 79.8 % [95 % I.C: 75.2, 84.7]; p = 0.006).
Limites de l’étude: La présente étude ne visait pas à évaluer de façon systématique l’impact d’un protocole de prévention sur l’incidence d’un épisode d’IRA, étant donné qu’elle s’est limitée aux paramètres établis dans un seul cadre régional.
Conclusion: L’incidence d’un épisode d’IRA chez les patients hospitalisés subissant un examen en tomodensitométrie demeure faible, et n’apparait pas significativement différente qu’ils reçoivent ou non un agent de contraste au préalable. Une surveillance plus rigoureuse des taux de créatinine sérique chez les patients à risque n’a pas non plus mené à des différences marquées dans l’incidence d’un épisode d’IRA post-scanner. Ainsi, une meilleure compréhension des facteurs susceptibles de provoquer des épisodes d’IRA post-scanner est requise afin d’améliorer les stratégies visant la réduction de leur incidence.
Figures
Similar articles
-
Plasma neutrophil gelatinase-associated lipocalin (NGAL) as an early predictive marker of contrast-induced nephropathy in hospitalized patients undergoing computed tomography.Clin Kidney J. 2013 Dec;6(6):578-83. doi: 10.1093/ckj/sft109. Epub 2013 Aug 28. Clin Kidney J. 2013. PMID: 26069825 Free PMC article.
-
Intravenous contrast material-induced nephropathy: causal or coincident phenomenon?Radiology. 2013 Apr;267(1):106-18. doi: 10.1148/radiol.12121823. Epub 2013 Jan 29. Radiology. 2013. PMID: 23360742 Free PMC article.
-
Intravenous contrast use and acute kidney injury: a retrospective study of 1,238 inpatients undergoing computed tomography.Radiol Bras. 2021 Mar-Apr;54(2):77-82. doi: 10.1590/0100-3984.2020.0018. Radiol Bras. 2021. PMID: 33854260 Free PMC article.
-
Is the risk of contrast-induced nephropathy a real contraindication to perform intravenous contrast enhanced Computed Tomography for non-traumatic acute abdomen in Emergency Surgery Department?Acta Biomed. 2018 Dec 17;89(9-S):158-172. doi: 10.23750/abm.v89i9-S.7891. Acta Biomed. 2018. PMID: 30561410 Free PMC article.
-
Neutrophil gelatinase-associated lipocalin (NGAL): a promising biomarker of contrast-induced nephropathy after computed tomography.Ren Fail. 2014 Jul;36(6):979-86. doi: 10.3109/0886022X.2014.900429. Epub 2014 Mar 27. Ren Fail. 2014. PMID: 24673459 Review.
Cited by
-
Contrast associated nephropathy after intravenous administration: what is the magnitude of the problem?Ren Fail. 2021 Dec;43(1):1311-1321. doi: 10.1080/0886022X.2021.1978490. Ren Fail. 2021. PMID: 34547972 Free PMC article. Review.
-
CT angiography for pulmonary embolism in the emergency department: investigation of a protocol by 20 ml of high-concentration contrast medium.Radiol Med. 2020 Feb;125(2):137-144. doi: 10.1007/s11547-019-01098-6. Epub 2019 Oct 28. Radiol Med. 2020. PMID: 31659676
-
Creatinine level variation in patients subjected to contrast-enhanced tomography: a meta-analysis.J Vasc Bras. 2021 Jul 5;20:e20200161. doi: 10.1590/1677-5449.200161. eCollection 2021. J Vasc Bras. 2021. PMID: 34267786 Free PMC article. Review.
-
Contrast-associated acute kidney injury is a myth: We are not sure.Intensive Care Med. 2018 Jan;44(1):110-114. doi: 10.1007/s00134-017-4970-2. Epub 2017 Dec 14. Intensive Care Med. 2018. PMID: 29242970 No abstract available.
-
Preoperative Assessment of Hepatocellular Carcinoma with Split-Bolus Combined Phase Contrast-Enhanced Computed Tomography.Med Sci Monit. 2017 Apr 16;23:1834-1841. doi: 10.12659/msm.904129. Med Sci Monit. 2017. PMID: 28412761 Free PMC article. Clinical Trial.
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. 2012;Suppl(2):1–138.
LinkOut - more resources
Full Text Sources
Other Literature Sources
