

Therapeutic options for management of endometrial hyperplasia
- PMID: 26463434
- PMCID: PMC4695458
- DOI: 10.3802/jgo.2016.27.e8
Therapeutic options for management of endometrial hyperplasia
Abstract
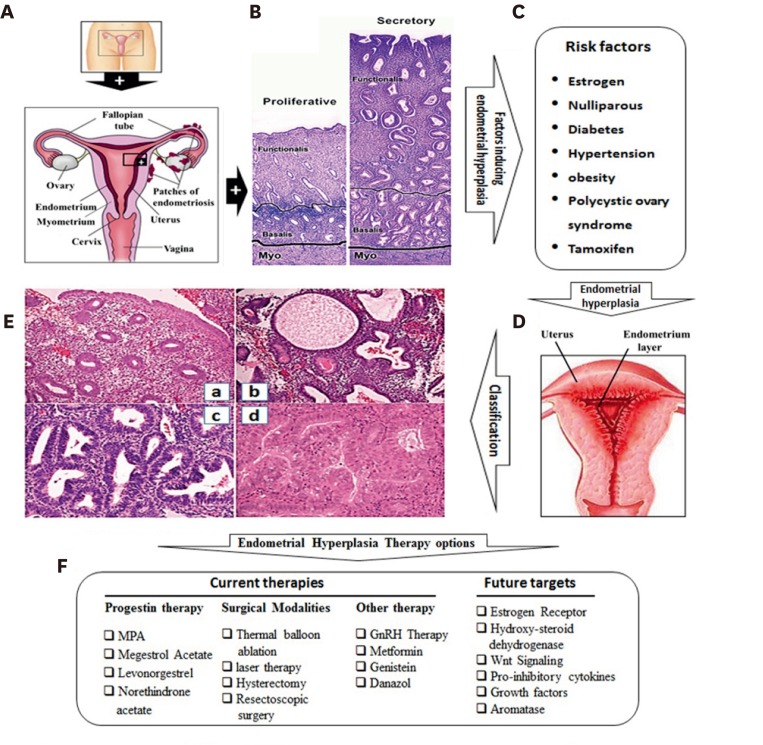
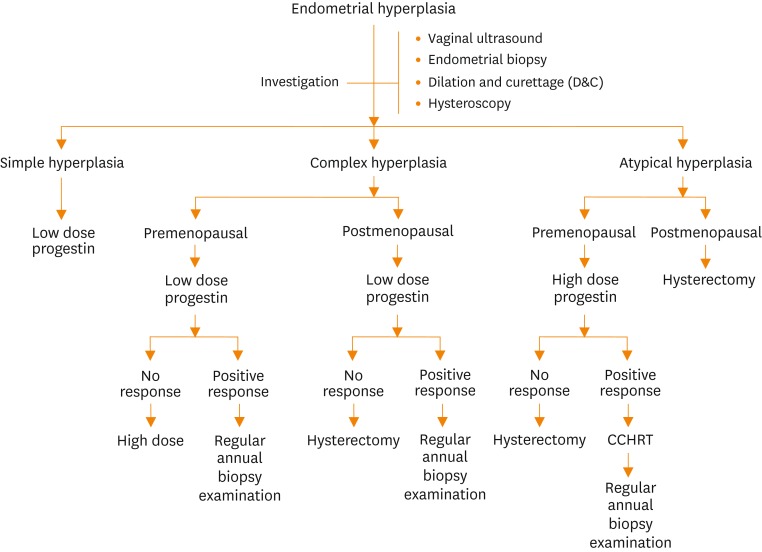
Endometrial hyperplasia (EH) comprises a spectrum of changes in the endometrium ranging from a slightly disordered pattern that exaggerates the alterations seen in the late proliferative phase of the menstrual cycle to irregular, hyperchromatic lesions that are similar to endometrioid adenocarcinoma. Generally, EH is caused by continuous exposure of estrogen unopposed by progesterone, polycystic ovary syndrome, tamoxifen, or hormone replacement therapy. Since it can progress, or often occur coincidentally with endometrial carcinoma, EH is of clinical importance, and the reversion of hyperplasia to normal endometrium represents the key conservative treatment for prevention of the development of adenocarcinoma. Presently, cyclic progestin or hysterectomy constitutes the major treatment option for EH without or with atypia, respectively. However, clinical trials of hormonal therapies and definitive standard treatments remain to be established for the management of EH. Moreover, therapeutic options for EH patients who wish to preserve fertility are challenging and require nonsurgical management. Therefore, future studies should focus on evaluation of new treatment strategies and novel compounds that could simultaneously target pathways involved in the pathogenesis of estradiol-induced EH. Novel therapeutic agents precisely targeting the inhibition of estrogen receptor, growth factor receptors, and signal transduction pathways are likely to constitute an optimal approach for treatment of EH.
Keywords: Endometrial Hyperplasia; Progestins; Receptors, Estrogen; Therapy.
Conflict of interest statement
Figures
References
-
- Jabbour HN, Kelly RW, Fraser HM, Critchley HO. Endocrine regulation of menstruation. Endocr Rev. 2006;27:17–46. - PubMed
-
- Horne FM, Blithe DL. Progesterone receptor modulators and the endometrium: changes and consequences. Hum Reprod Update. 2007;13:567–580. - PubMed
-
- Kaaks R, Lukanova A, Kurzer MS. Obesity, endogenous hormones, and endometrial cancer risk: a synthetic review. Cancer Epidemiol Biomarkers Prev. 2002;11:1531–1543. - PubMed
-
- Horn LC, Schnurrbusch U, Bilek K, Hentschel B, Einenkel J. Risk of progression in complex and atypical endometrial hyperplasia: clinicopathologic analysis in cases with and without progestogen treatment. Int J Gynecol Cancer. 2004;14:348–353. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
