

T-cell Exhaustion in Multiple Myeloma Relapse after Autotransplant: Optimal Timing of Immunotherapy
- PMID: 26464015
- PMCID: PMC4703436
- DOI: 10.1158/2326-6066.CIR-15-0055
T-cell Exhaustion in Multiple Myeloma Relapse after Autotransplant: Optimal Timing of Immunotherapy
Abstract
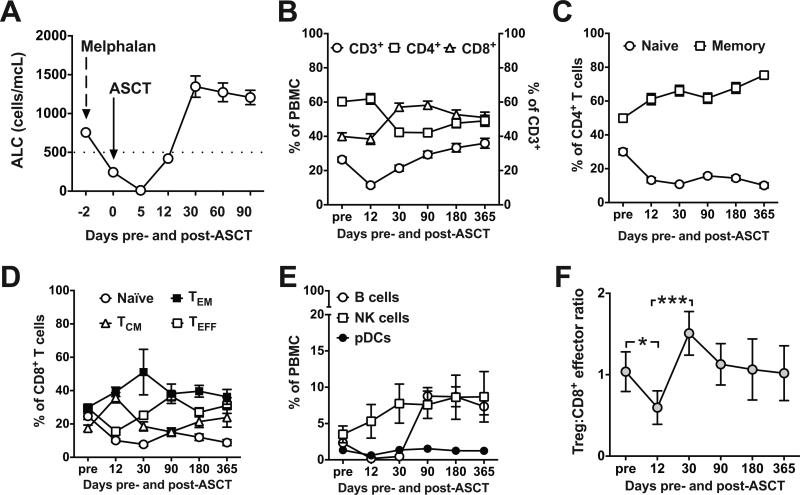
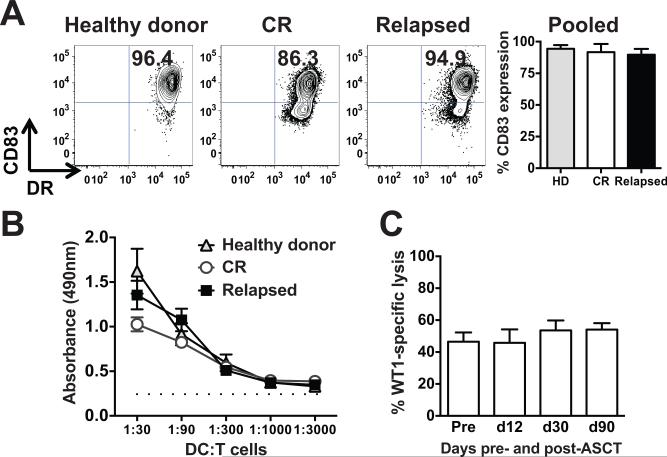
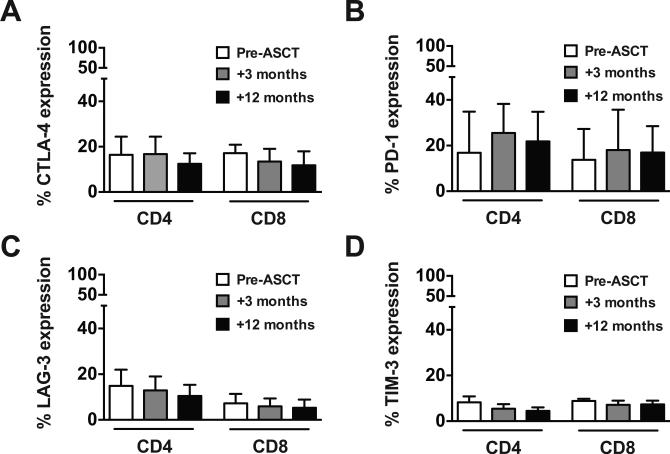
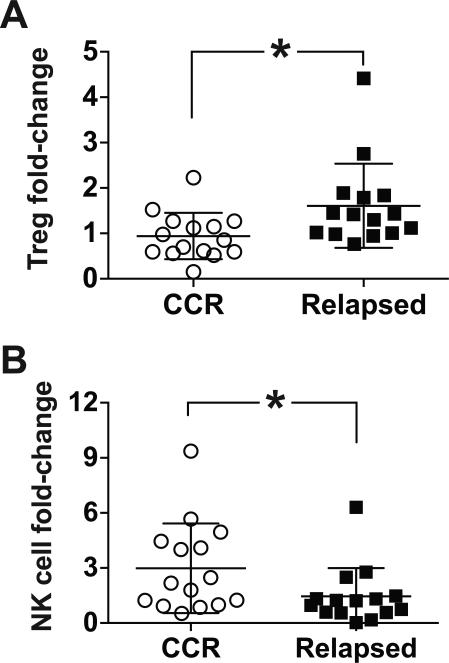
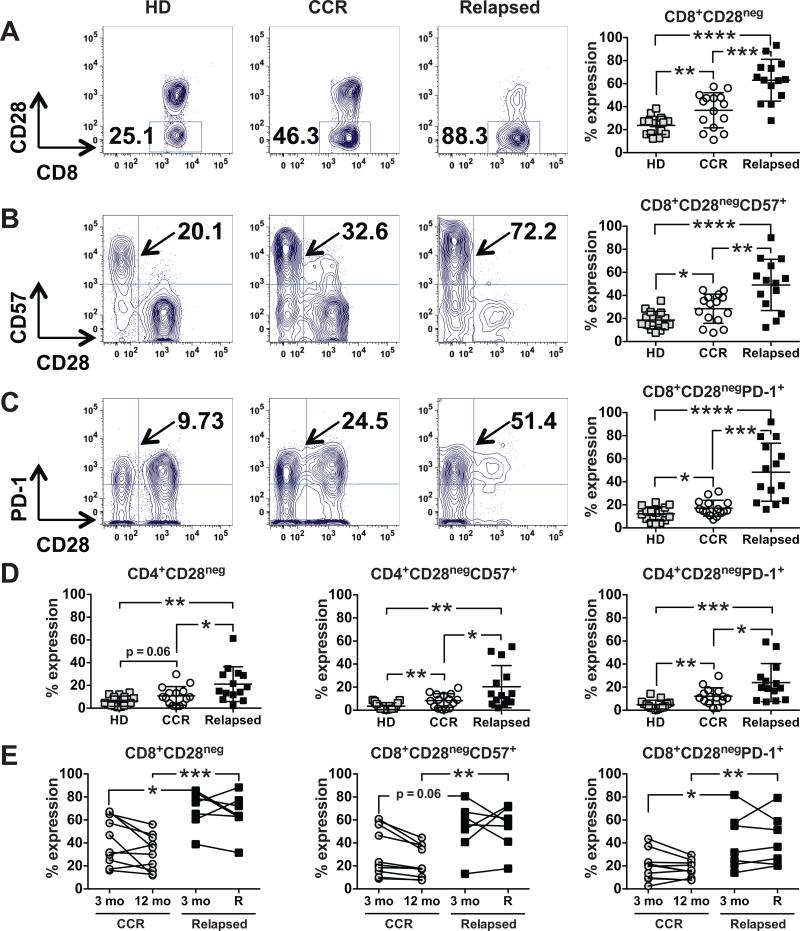
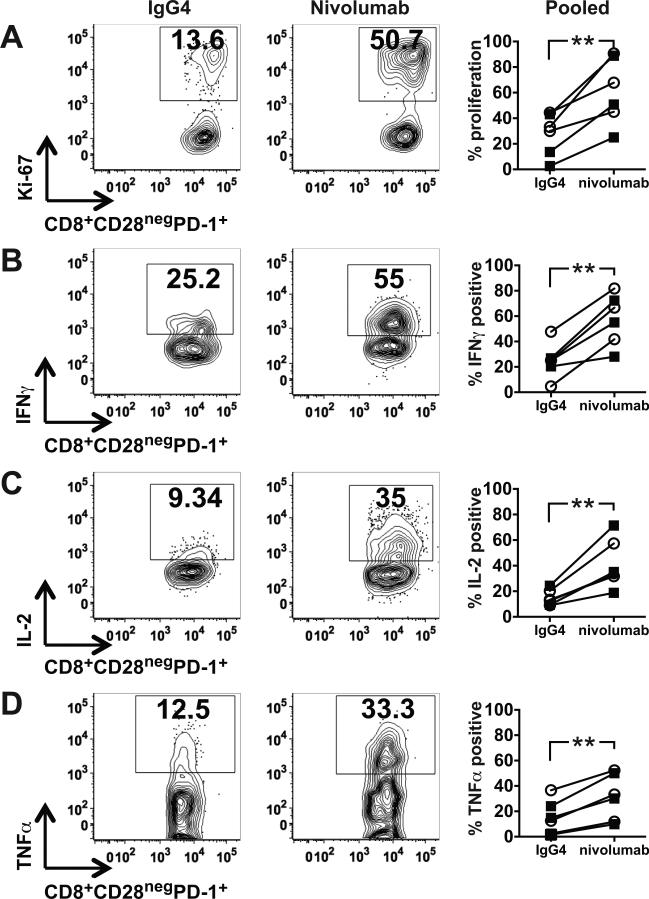
Multiple myeloma is the most common indication for high-dose chemotherapy and autologous stem cell transplantation (ASCT), and lenalidomide maintenance after transplant is now standard. Although lenalidomide doubles progression-free survival, almost all patients eventually relapse. Posttransplant immunotherapy to improve outcomes after ASCT therefore has great merit but first requires delineation of the dynamics of immune reconstitution. We evaluated lymphocyte composition and function after ASCT to guide optimal timing of immunotherapy and to identify potential markers of relapse. Regulatory T cells (Treg) decline as CD8(+) T cells expand during early lymphocyte recovery after ASCT, markedly reducing the Treg:CD8(+) effector T-cell ratio. These CD8(+) T cells can respond to autologous dendritic cells presenting tumor antigen in vitro as early as day +12 after transplant, becoming antigen-specific cytolytic T-lymphocyte effectors and thereby demonstrating preservation of cellular reactivity. CD4(+) and CD8(+) T cells express the negative regulatory molecules, CTLA-4, PD-1, LAG-3, and TIM-3, before and after ASCT. A subpopulation of exhausted/senescent CD8(+) T cells, however, downregulates CD28 and upregulates CD57 and PD-1, characterizing immune impairment and relapse after ASCT. Relapsing patients have higher numbers of these cells at +3 months after transplant, but before detection of clinical disease, indicating their applicability in identifying patients at higher risk of relapse. PD-1 blockade also revives the proliferation and cytokine secretion of the hyporesponsive, exhausted/senescent CD8(+) T cells in vitro. Collectively, these results identify T-cell exhaustion/senescence as a distinguishing feature of relapse and support early introduction of immunotherapy to stimulate antitumor immunity after ASCT.
©2015 American Association for Cancer Research.
Figures
References
-
- Attal M, Lauwers-Cances V, Marit G, Caillot D, Moreau P, Facon T, et al. Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N Engl J Med. 2012;366(19):1782–91. - PubMed
-
- Palumbo A, Cavallo F, Gay F, Di Raimondo F, Ben Yehuda D, Petrucci MT, et al. Autologous transplantation and maintenance therapy in multiple myeloma. N Engl J Med. 2014;371(10):895–905. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
