

Comparison of risk stratification tools in predicting outcomes of patients with higher-risk myelodysplastic syndromes treated with azanucleosides
- PMID: 26464171
- PMCID: PMC4775363
- DOI: 10.1038/leu.2015.283
Comparison of risk stratification tools in predicting outcomes of patients with higher-risk myelodysplastic syndromes treated with azanucleosides
Abstract
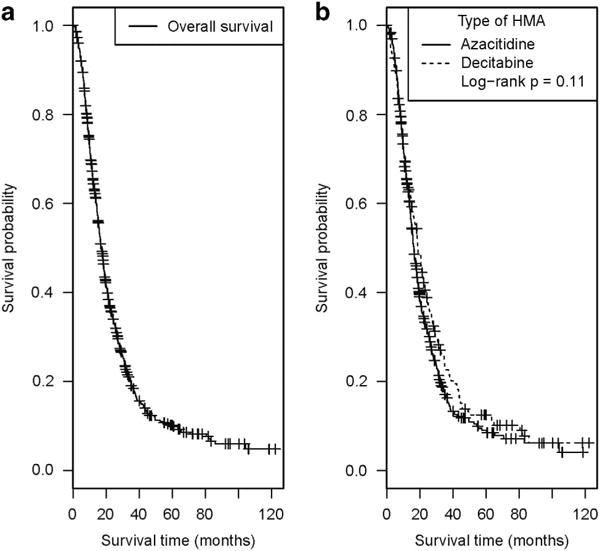
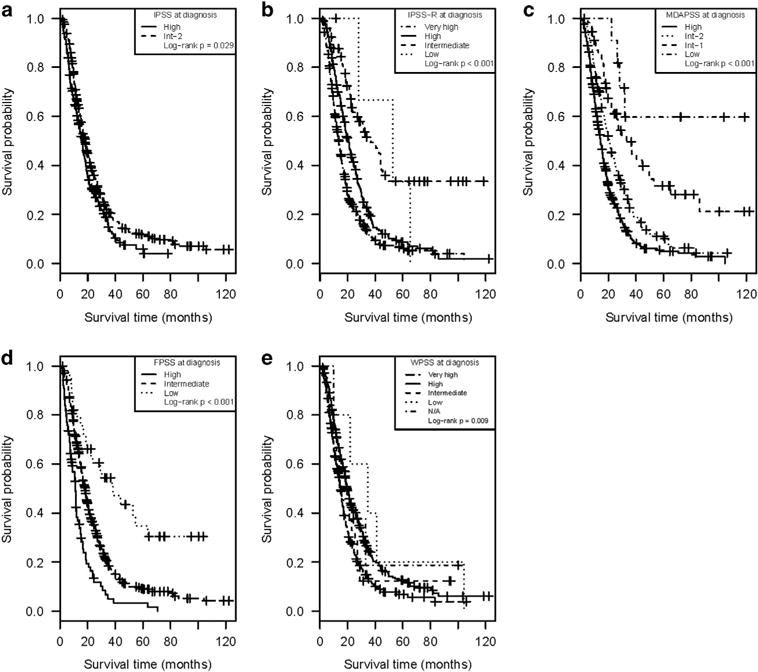
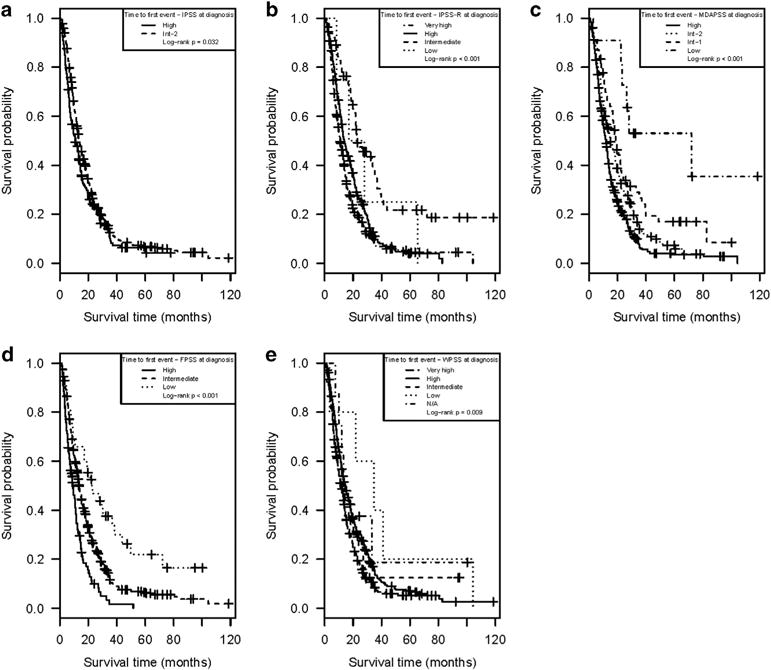
Established prognostic tools in patients with myelodysplastic syndromes (MDS) were largely derived from untreated patient cohorts. Although azanucleosides are standard therapies for higher-risk (HR)-MDS, the relative prognostic performance of existing prognostic tools among patients with HR-MDS receiving azanucleoside therapy is unknown. In the MDS Clinical Research Consortium database, we compared the prognostic utility of the International Prognostic Scoring System (IPSS), revised IPSS (IPSS-R), MD Anderson Prognostic Scoring System (MDAPSS), World Health Organization-based Prognostic Scoring System (WPSS) and the French Prognostic Scoring System (FPSS) among 632 patients who presented with HR-MDS and were treated with azanucleosides as the first-line therapy. Median follow-up from diagnosis was 15.7 months. No prognostic tool predicted the probability of achieving an objective response. Nonetheless, all five tools were associated with overall survival (OS, P=0.025 for the IPSS, P=0.011 for WPSS and P<0.001 for the other three tools). The corrected Akaike Information Criteria, which were used to compare OS with the different prognostic scoring systems as covariates (lower is better) were 4138 (MDAPSS), 4156 (FPSS), 4196 (IPSS-R), 4186 (WPSS) and 4196 (IPSS). Patients in the highest-risk groups of the prognostic tools had a median OS from diagnosis of 11-16 months and should be considered for up-front transplantation or experimental approaches.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tefferi A, Vardiman JW. Myelodysplastic syndromes. N Engl J Med. 2009;361:1872–1885. - PubMed
-
- Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009;114:937–951. - PubMed
-
- Raza A, Galili N. The genetic basis of phenotypic heterogeneity in myelodysplastic syndromes. Nat Rev Cancer. 2012;12:849–859. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
