

Total esophagogastrectomy plus extended lymphadenectomy with transverse colon interposition: A treatment for extensive esophagogastric junction cancer
- PMID: 26464757
- PMCID: PMC4598612
- DOI: 10.4254/wjh.v7.i22.2411
Total esophagogastrectomy plus extended lymphadenectomy with transverse colon interposition: A treatment for extensive esophagogastric junction cancer
Abstract
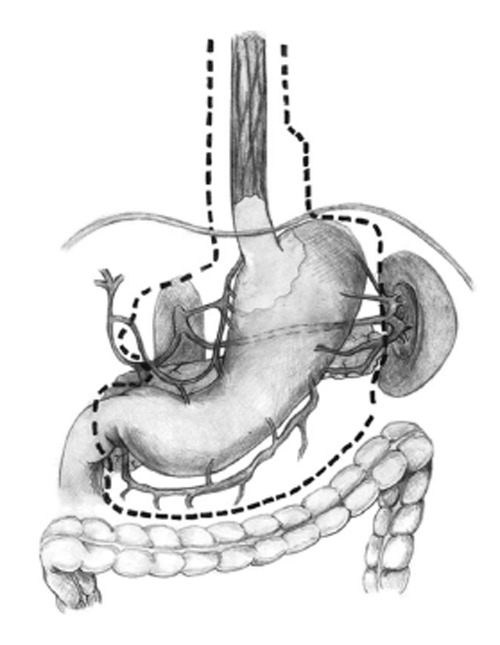
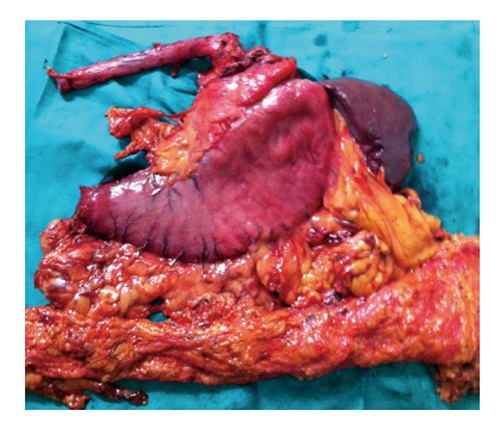
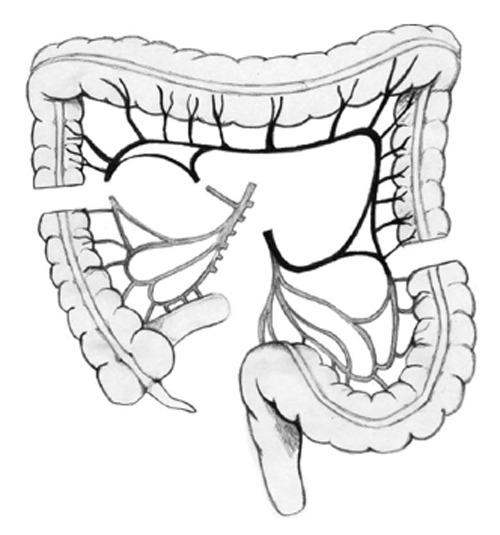
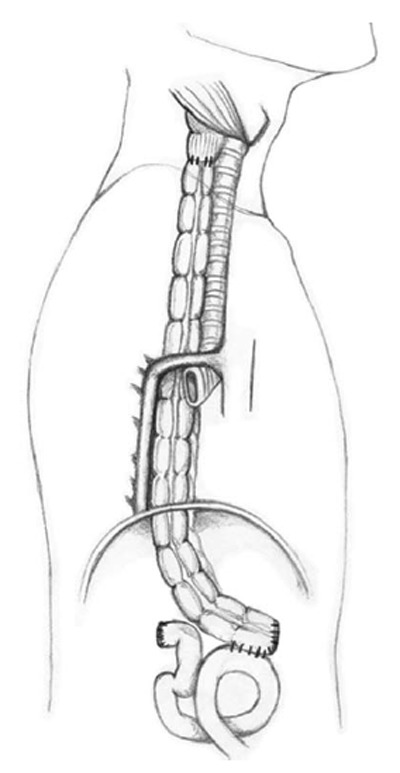
Aim: To review the post-operative morbidity and mortality of total esophagogastrectomy (TEG) with second barrier lymphadenectomy (D2) with interposition of a transverse colon and to determine the oncological outcomes of TEG D2 with interposition of a transverse colon.
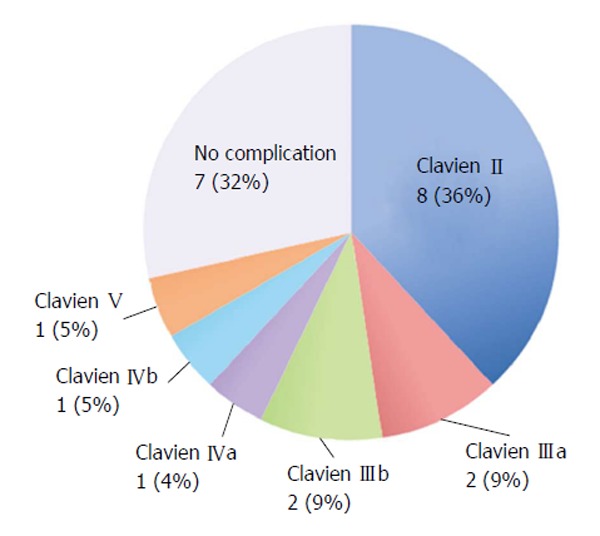
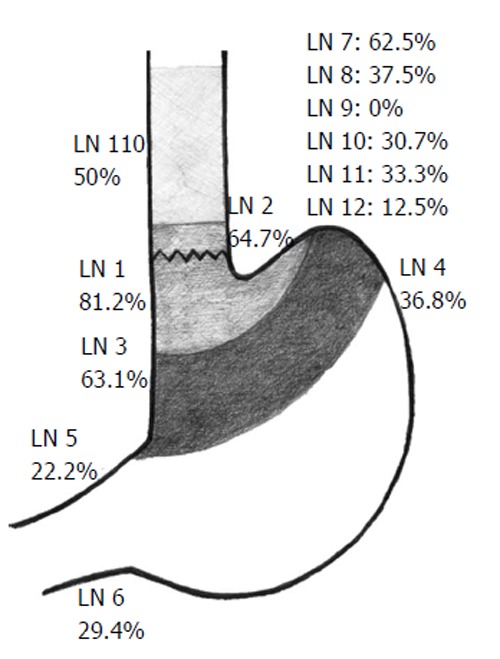
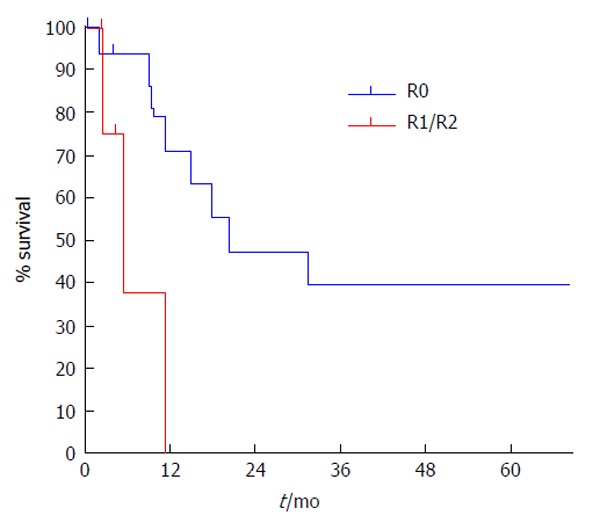
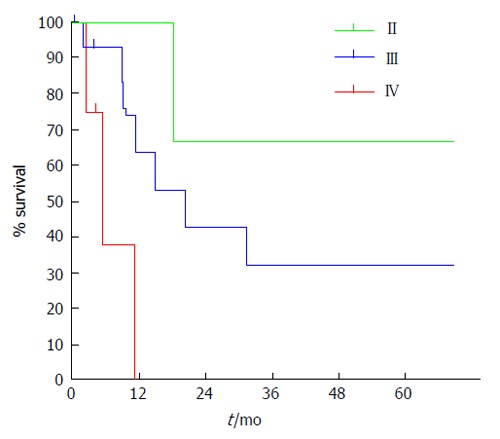
Methods: This study consisted of a retrospective review of patients with a cancer diagnosis who underwent TEG between 1997 and 2013. Demographic data, surgery protocols, complications according to Clavien-Dindo classifications, final pathological reports, oncological follow-ups and causes of death were recorded. We used the TNM 2010 and Japanese classifications for nodal dissection of gastric cancer. We used descriptive statistical analysis and Kaplan-Meier survival curves. A P-value of less than 0.05 was considered statistically significant.
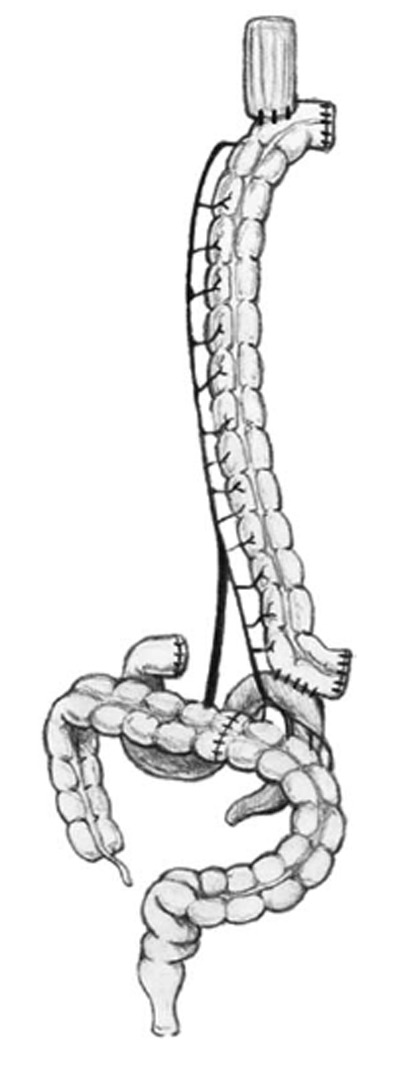
Results: The series consisted of 21 patients (80.9% men). The median age was 60 years. The 2 main surgical indications were extensive esophagogastric junction cancers (85.7%) and double cancers (14.2%). The mean total surgery time was 405 min (352-465 min). Interposition of a transverse colon through the posterior mediastinum was used for replacement in all cases. Splenectomy was required in 13 patients (61.9%), distal pancreatectomy was required in 2 patients (9.5%) and resection of the left adrenal gland was required in 1 patient (4.7%). No residual cancer surgery was achieved in 75.1% of patients. A total of 71.4% of patients had a postoperative complication. Respiratory complications were the most frequently observed complication. Postoperative mortality was 5.8%. Median follow-up was 13.4 mo. Surgery specific survival at 5 years of follow-up was 32.8%; for patients with curative surgery, it was 39.5% at 5 years.
Conclusion: TEG for cancer with interposition of a transverse colon is a very complex surgery, and it presents high post-operative morbidity and adequate oncological outcomes.
Keywords: Esophagogastric junction cancer; Total esophagectomy; Total esophagogastrectomy; Total gastrectomy; Transverse colon interposition.
Figures
References
-
- Vial M, Grande L, Pera M. Epidemiology of adenocarcinoma of the esophagus, gastric cardia, and upper gastric third. Recent Results Cancer Res. 2010;182:1–17. - PubMed
-
- Blot WJ, Devesa SS, Kneller RW, Fraumeni JF. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991;265:1287–1289. - PubMed
-
- Pera M, Cameron AJ, Trastek VF, Carpenter HA, Zinsmeister AR. Increasing incidence of adenocarcinoma of the esophagus and esophagogastric junction. Gastroenterology. 1993;104:510–513. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–2053. - PubMed
-
- Whitson BA, Groth SS, Li Z, Kratzke RA, Maddaus MA. Survival of patients with distal esophageal and gastric cardia tumors: a population-based analysis of gastroesophageal junction carcinomas. J Thorac Cardiovasc Surg. 2010;139:43–48. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
