

CHROMOBLASTOMYCOSIS: A NEGLECTED TROPICAL DISEASE
- PMID: 26465369
- PMCID: PMC4711190
- DOI: 10.1590/S0036-46652015000700009
CHROMOBLASTOMYCOSIS: A NEGLECTED TROPICAL DISEASE
Abstract
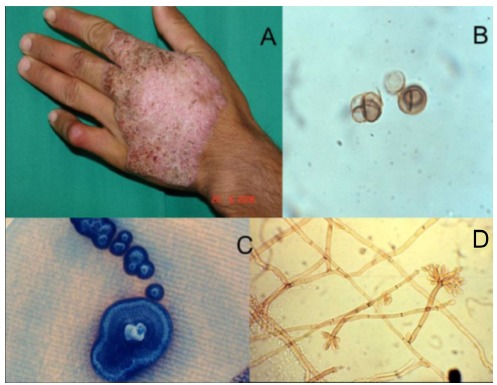
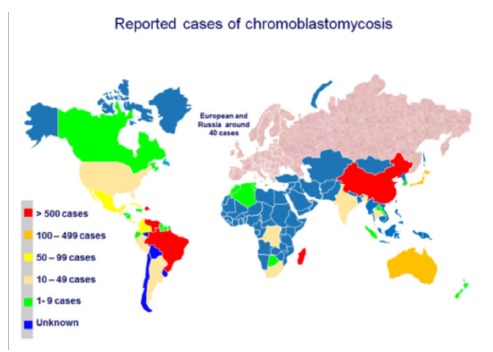
Chromoblastomycosis (CMB) is a chronic fungal infection of the skin and the subcutaneous tissue caused by a transcutaneous traumatic inoculation of a specific group of dematiaceous fungi occurring mainly in tropical and subtropical zones worldwide. If not diagnosed at early stages, patients with CBM require long term therapy with systemic antifungals, sometimes associated with physical methods. Unlike other neglected endemic mycoses, comparative clinical trials have not been performed for this disease. Nowadays, therapy is based on a few open trials and on expert opinion. Itraconazole either as monotherapy or associated with other drugs, or with physical methods, is widely used. Recently, photodynamic therapy has been successfully employed in combination with antifungals in patients presenting with CBM. In the present revision the most used therapeutic options against CBM are reviewed as well as the several factors that may have impact on the patient's outcome.
Cromoblastomicose (CMB) é uma infecção fúngica crônica da pele e tecido subcutâneo causada pela inoculação transcutânea traumática de um grupo específico de fungos dermatiáceos que ocorrem principalmente em zonas tropicais e subtropicais do mundo. Quando não são diagnosticados nas fases iniciais, pacientes com CBM necessitam de tratamentos prolongados com antifúngicos sistêmicos, por vezes associados a métodos físicos. Diferentemente de outras micoses endêmicas negligenciadas, não foram realizados ensaios clínicos comparativos para esta doença. Atualmente a terapia é baseada em alguns poucos ensaios abertos e em opiniões de especialistas. Itraconazol é amplamente utilizado como monoterapia ou em associação com outras drogas, ou com métodos físicos. Recentemente, a terapia fotodinâmica foi empregada com sucesso combinada a antifúngicos em pacientes com CBM. Neste manuscrito as opções terapêuticas mais utilizadas contra CBM foram revistas, assim como os diversos fatores que podem influenciar a evolução dos pacientes
Figures



Similar articles
-
Challenges in the therapy of chromoblastomycosis.Mycopathologia. 2013 Jun;175(5-6):477-88. doi: 10.1007/s11046-013-9648-x. Epub 2013 May 2. Mycopathologia. 2013. PMID: 23636730 Review.
-
Chromoblastomycosis and sporotrichosis, two endemic but neglected fungal infections in Madagascar.J Mycol Med. 2017 Sep;27(3):312-324. doi: 10.1016/j.mycmed.2017.08.003. Epub 2017 Aug 25. J Mycol Med. 2017. PMID: 28847419 Review.
-
Treatment of chromoblastomycosis with itraconazole, cryosurgery, and a combination of both.Int J Dermatol. 1997 Jul;36(7):542-7. doi: 10.1046/j.1365-4362.1997.00085.x. Int J Dermatol. 1997. PMID: 9268758 Clinical Trial.
-
Chromoblastomycosis.Clin Microbiol Rev. 2017 Jan;30(1):233-276. doi: 10.1128/CMR.00032-16. Clin Microbiol Rev. 2017. PMID: 27856522 Free PMC article. Review.
-
Managing chromoblastomycosis.Trop Doct. 2010 Apr;40(2):65-7. doi: 10.1258/td.2009.090264. Trop Doct. 2010. PMID: 20305094 Review.
Cited by
-
The Current Landscape of Repurposed Drugs for Fungal Neglected Tropical Diseases.Curr Fungal Infect Rep. 2025 Dec;19(1):7. doi: 10.1007/s12281-025-00504-z. Epub 2025 May 29. Curr Fungal Infect Rep. 2025. PMID: 40837073 Free PMC article.
-
Arthrocladium fulminans Arthritis and Osteomyelitis.Am J Trop Med Hyg. 2017 Mar;96(3):698-700. doi: 10.4269/ajtmh.16-0185. Epub 2017 Apr 6. Am J Trop Med Hyg. 2017. PMID: 28070004 Free PMC article.
-
Modulation of the immune response by Fonsecaea pedrosoi morphotypes in the course of experimental chromoblastomycosis and their role on inflammatory response chronicity.PLoS Negl Trop Dis. 2017 Mar 29;11(3):e0005461. doi: 10.1371/journal.pntd.0005461. eCollection 2017 Mar. PLoS Negl Trop Dis. 2017. PMID: 28355277 Free PMC article.
-
Fungal Infections of Implantation: More Than Five Years of Cases of Subcutaneous Fungal Infections Seen at the UK Mycology Reference Laboratory.J Fungi (Basel). 2022 Mar 25;8(4):343. doi: 10.3390/jof8040343. J Fungi (Basel). 2022. PMID: 35448574 Free PMC article.
-
Photodynamic Therapy for the Treatment of Fungal Infections.Infect Drug Resist. 2022 Jun 21;15:3251-3266. doi: 10.2147/IDR.S369605. eCollection 2022. Infect Drug Resist. 2022. PMID: 35761978 Free PMC article. Review.
References
-
- AL-DOORY Y. Di Salvo AF. Occupational mycoses. Philadelphia: Lea & Febiger; 1983. Chromomycosis; pp. 95–121.
-
- Antonello VS, Appel da Silva MC, Cambruzzi E, Kliemann DA, Santos BR, Queiroz-Telles F. Treatment of severe chromoblastomycosis with itraconazole and 5-flucytosine association. Rev Inst Med Trop Sao Paulo. 2010;52:329–331. - PubMed
-
- Attapattu MC. Chromoblastomycosis: a clinical and mycological study of 71 cases from Sri Lanka. Mycopathologia. 1997;137:145–151. - PubMed
-
- Avelar-Pires C, Simoes-Quaresma JA, Moraes de Macedo GM, Brasil-Xavier M, Cardoso de Brito A. Revisiting the clinical and histopathological aspects of patients with chromoblastomycosis from the Brazilian Amazon region. Arch Med Res. 2013;44:302–306. - PubMed
-
- Bolzinger T, Pradinaud R, Sainte-Marie D, Dupont B, Chwetzoff E. Traitement de quatre cas de chromomycose àFonsecaea pedrosoipar l'association 5-fluorocytosine-itraconazole. Nouv Dermatol. 1991;10:462–466.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
