

Percutaneous Balloon Compression vs Percutaneous Retrogasserian Glycerol Rhizotomy for the Primary Treatment of Trigeminal Neuralgia
- PMID: 26465639
- PMCID: PMC4747977
- DOI: 10.1227/NEU.0000000000001059
Percutaneous Balloon Compression vs Percutaneous Retrogasserian Glycerol Rhizotomy for the Primary Treatment of Trigeminal Neuralgia
Abstract
Background: Despite >30 years of clinical use, the literature is still sparse when it comes to comparisons between percutaneous balloon compression (PBC) and percutaneous retrogasserian glycerol rhizolysis (PRGR) as treatments for trigeminal neuralgia.
Objective: To perform a retrospective cohort comparison between PBC and PRGR with regard to therapeutic effect, side effects, and complications.
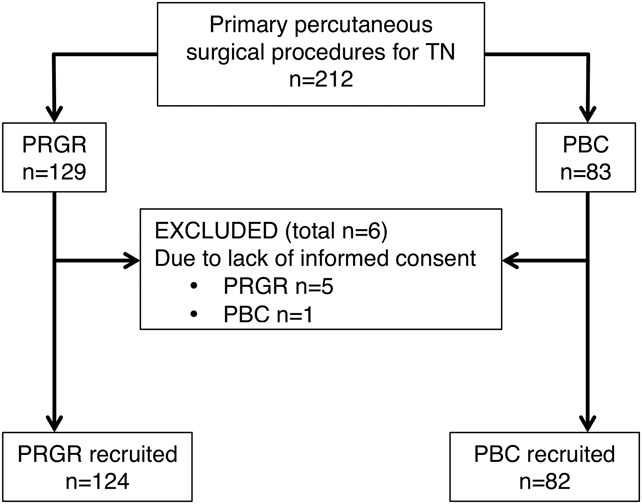
Methods: Medical records and follow-up data from 124 primary PRGRs performed from 1986 to 2000 and 82 primary PBCs performed from 2000 to 2013 were reviewed. All patients had undergone clinical sensory testing and assessment of sensory thresholds. Analyses were performed to compare duration of pain relief, frequency of sensory disturbances, and side effects.
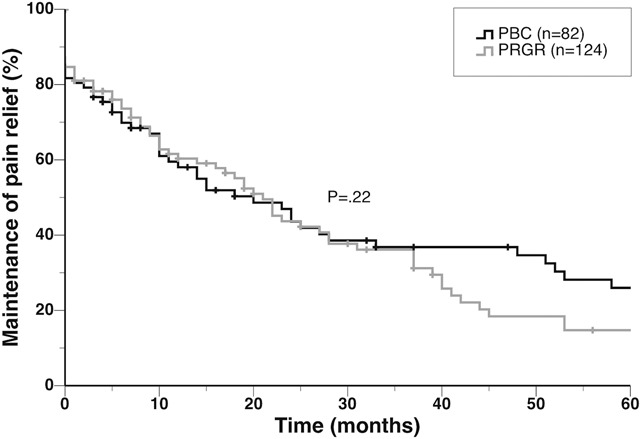
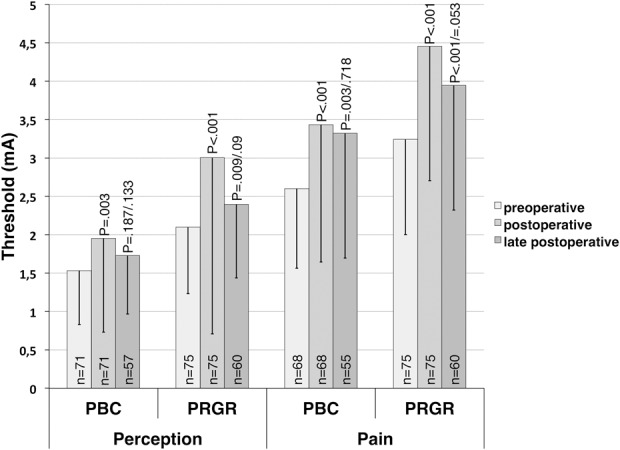
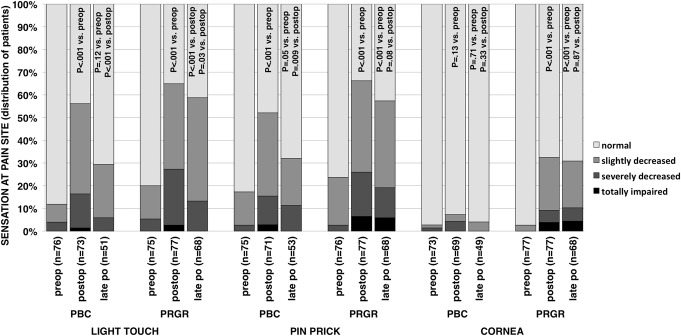
Results: Median duration of pain relief was 21 months after PRGR and 20 months after PBC. Both methods carried a high risk of hypesthesia/hypalgesia (P < .001) that was partly reversed with time. Decreased corneal sensibility was common after PRGR (P < .001) but not after PBC. Dysesthesia was more common after PRGR (23%) compared after PBC (4%; P < .001). Other side effects were noted but uncommon.
Conclusion: PBC and PRGR are both effective as primary surgical treatment of trigeminal neuralgia. Both carry a risk of postoperative hypesthesia, but in this series, the side effect profile favored PBC. Furthermore, PBC is technically less challenging, whereas PRGR requires fewer resources. Between these 2 techniques, we propose PBC as the primary surgical technique for percutaneous treatment of trigeminal neuralgia on the basis of its lower incidence of dysesthesia, corneal hypesthesia, and technical failures.
Figures
Comment in
-
Commentary: Percutaneous Balloon Compression vs Percutaneous Retrogasserian Glycerol Rhizotomy for the Primary Treatment of Trigeminal Neuralgia.Neurosurgery. 2016 Sep;79(3):E514. doi: 10.1227/NEU.0000000000001343. Neurosurgery. 2016. PMID: 27409405 No abstract available.
References
-
- Wilkins R. Trigeminal neuralgia: historical overview, with emphasis on surgical treatment. In: Burchiel K, ed. Surgical Management of Pain. New York, NY: Thieme; 2002:288-301.
-
- Håkanson S. Trigeminal neuralgia treated by the injection of glycerol into the trigeminal cistern. Neurosurgery. 1981;9(6):638-646. - PubMed
-
- Mullan S, Lichtor T. Percutaneous microcompression of the trigeminal ganglion for trigeminal neuralgia. J Neurosurg. 1983;59(6):1007-1012. - PubMed
-
- Kouzounias K, Lind G, Schechtmann G, Winter J, Linderoth B. Comparison of percutaneous balloon compression and glycerol rhizotomy for the treatment of trigeminal neuralgia. J Neurosurg. 2010;113(3):486-492. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
