

Neonatal Glycemia and Neurodevelopmental Outcomes at 2 Years
- PMID: 26465984
- PMCID: PMC4646166
- DOI: 10.1056/NEJMoa1504909
Neonatal Glycemia and Neurodevelopmental Outcomes at 2 Years
Abstract
Background: Neonatal hypoglycemia is common and can cause neurologic impairment, but evidence supporting thresholds for intervention is limited.
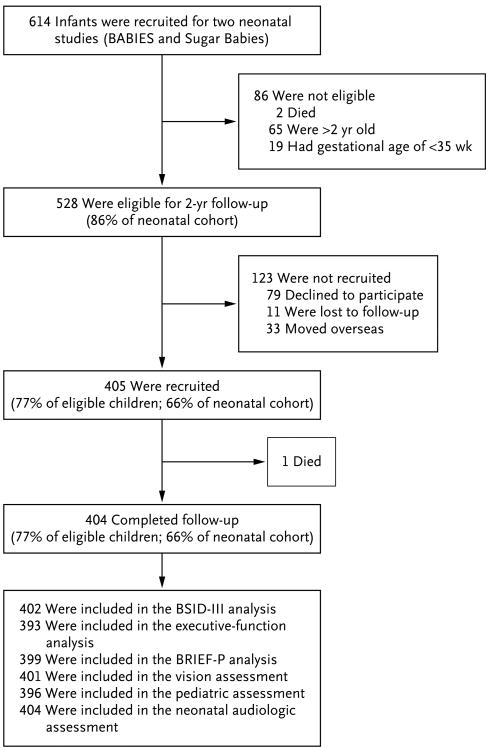
Methods: We performed a prospective cohort study involving 528 neonates with a gestational age of at least 35 weeks who were considered to be at risk for hypoglycemia; all were treated to maintain a blood glucose concentration of at least 47 mg per deciliter (2.6 mmol per liter). We intermittently measured blood glucose for up to 7 days. We continuously monitored interstitial glucose concentrations, which were masked to clinical staff. Assessment at 2 years included Bayley Scales of Infant Development III and tests of executive and visual function.
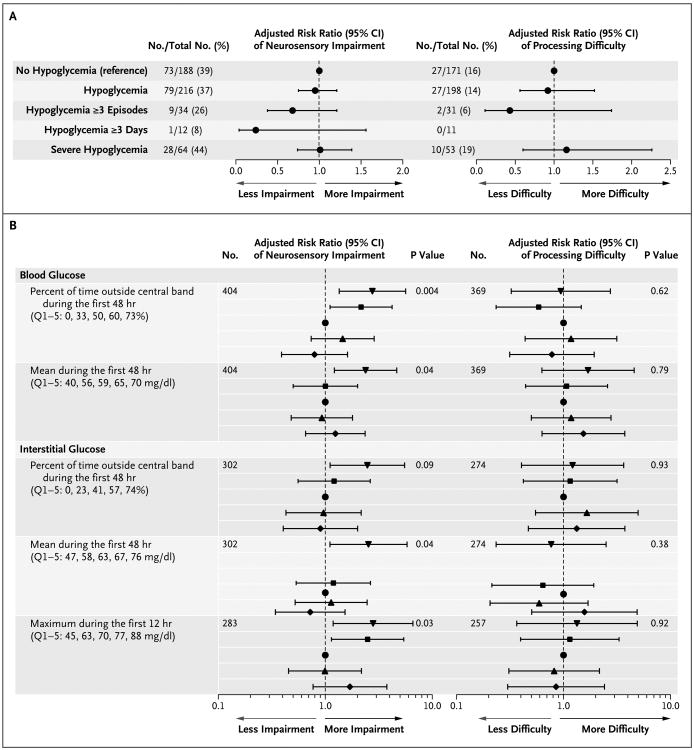
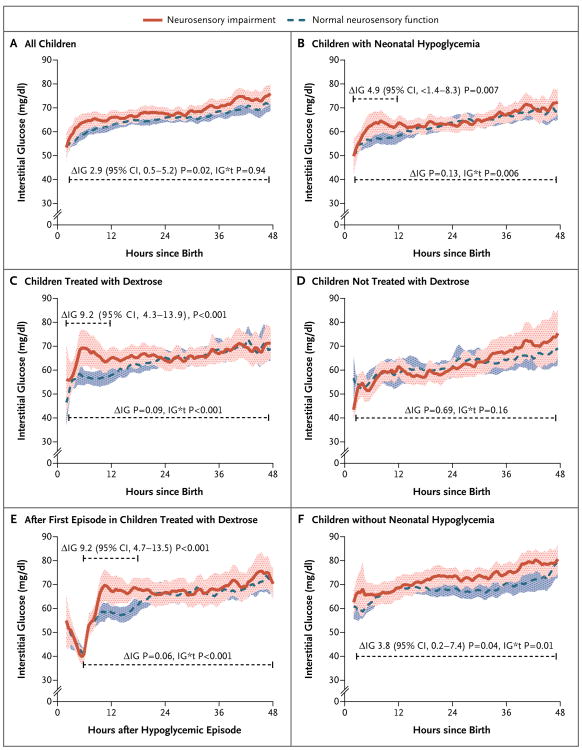
Results: Of 614 children, 528 were eligible, and 404 (77% of eligible children) were assessed; 216 children (53%) had neonatal hypoglycemia (blood glucose concentration, <47 mg per deciliter). Hypoglycemia, when treated to maintain a blood glucose concentration of at least 47 mg per deciliter, was not associated with an increased risk of the primary outcomes of neurosensory impairment (risk ratio, 0.95; 95% confidence interval [CI], 0.75 to 1.20; P=0.67) and processing difficulty, defined as an executive-function score or motion coherence threshold that was more than 1.5 SD from the mean (risk ratio, 0.92; 95% CI, 0.56 to 1.51; P=0.74). Risks were not increased among children with unrecognized hypoglycemia (a low interstitial glucose concentration only). The lowest blood glucose concentration, number of hypoglycemic episodes and events, and negative interstitial increment (area above the interstitial glucose concentration curve and below 47 mg per deciliter) also did not predict the outcome.
Conclusions: In this cohort, neonatal hypoglycemia was not associated with an adverse neurologic outcome when treatment was provided to maintain a blood glucose concentration of at least 47 mg per deciliter. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and others.).
Figures
Comment in
-
Neonatal Hypoglycemia Studies--Is There a Sweet Story of Success Yet?N Engl J Med. 2015 Oct 15;373(16):1567-9. doi: 10.1056/NEJMe1511994. N Engl J Med. 2015. PMID: 26465991 No abstract available.
-
Paediatric endocrinology: Defining treatment thresholds for neonatal hypoglycaemia-how low is too low?Nat Rev Endocrinol. 2015 Dec;11(12):687. doi: 10.1038/nrendo.2015.188. Epub 2015 Nov 3. Nat Rev Endocrinol. 2015. PMID: 26525878 No abstract available.
-
Neonates at risk for hypoglycemia: associated neurological outcomes.J Pediatr. 2016 Mar;170:343-4. doi: 10.1016/j.jpeds.2015.12.057. J Pediatr. 2016. PMID: 26922771 No abstract available.
References
-
- Burns CM, Rutherford MA, Boardman JP, Cowan FM. Patterns of cerebral injury and neurodevelopmental outcomes after symptomatic neonatal hypoglycemia. Pediatrics. 2008;122:65–74. - PubMed
-
- Boluyt N, van Kempen A, Offringa M. Neurodevelopment after neonatal hypoglycemia: a systematic review and design of an optimal future study. Pediatrics. 2006;117:2231–43. - PubMed
-
- Adamkin DH. Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics. 2011;127:575–9. - PubMed
-
- Harris DL, Weston PJ, Harding JE. Incidence of neonatal hypoglycemia in babies identified as at risk. J Pediatr. 2012;161:787–91. - PubMed
-
- March of Dimes Perinatal Data Center. Special care nursery admissions. 2011 http://www.marchofdimes.org/peristats/pdfdocs/nicu_summary_final.pdf.