

Topological data analysis for discovery in preclinical spinal cord injury and traumatic brain injury
- PMID: 26466022
- PMCID: PMC4634208
- DOI: 10.1038/ncomms9581
Topological data analysis for discovery in preclinical spinal cord injury and traumatic brain injury
Abstract
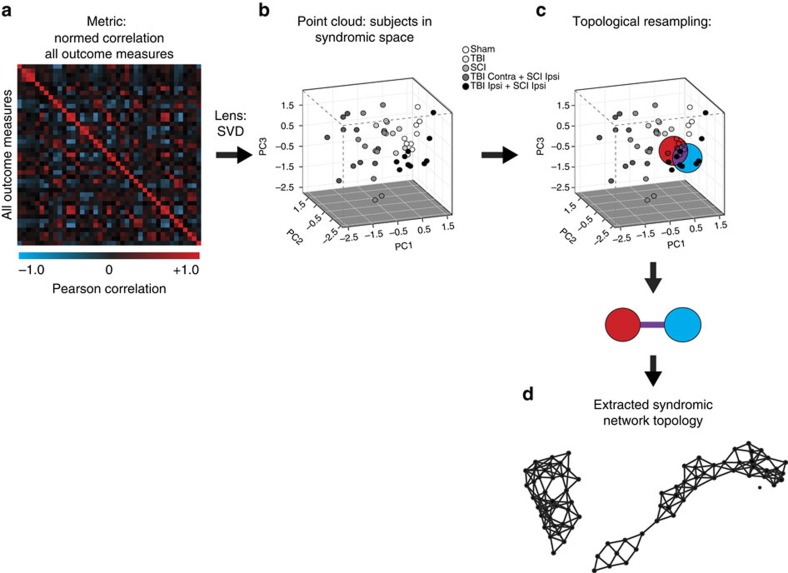
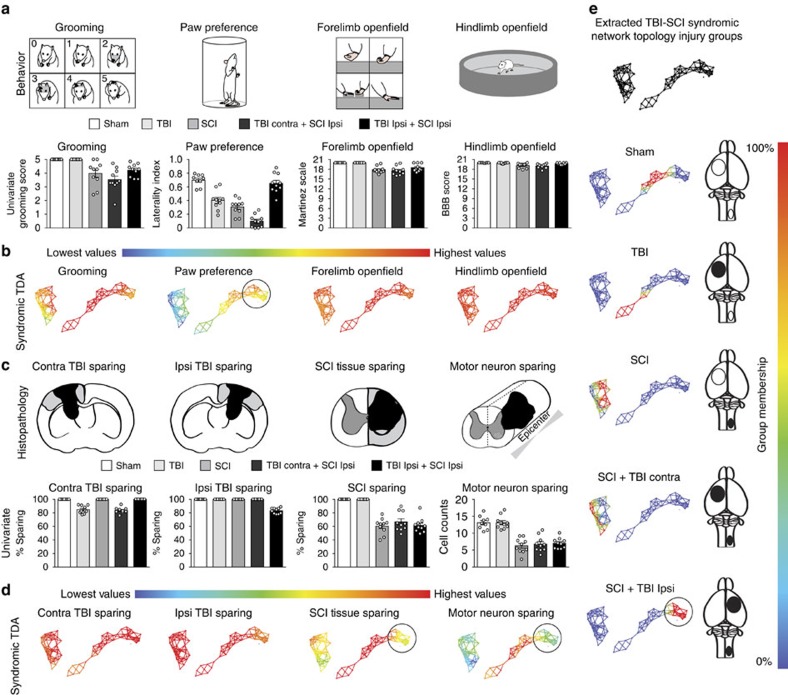
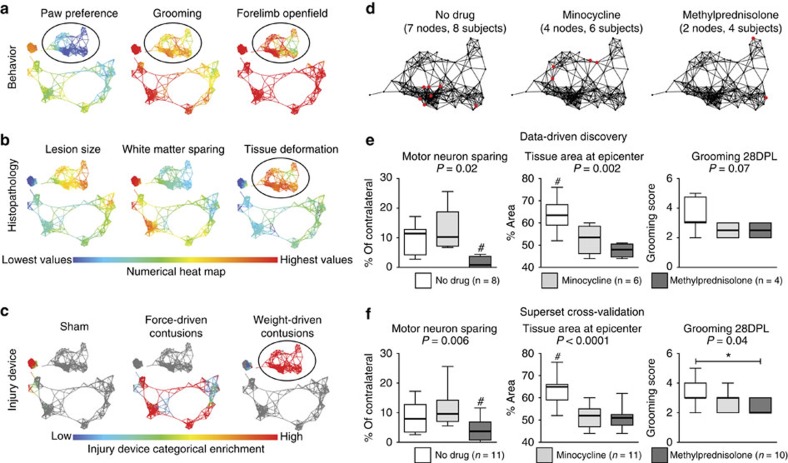
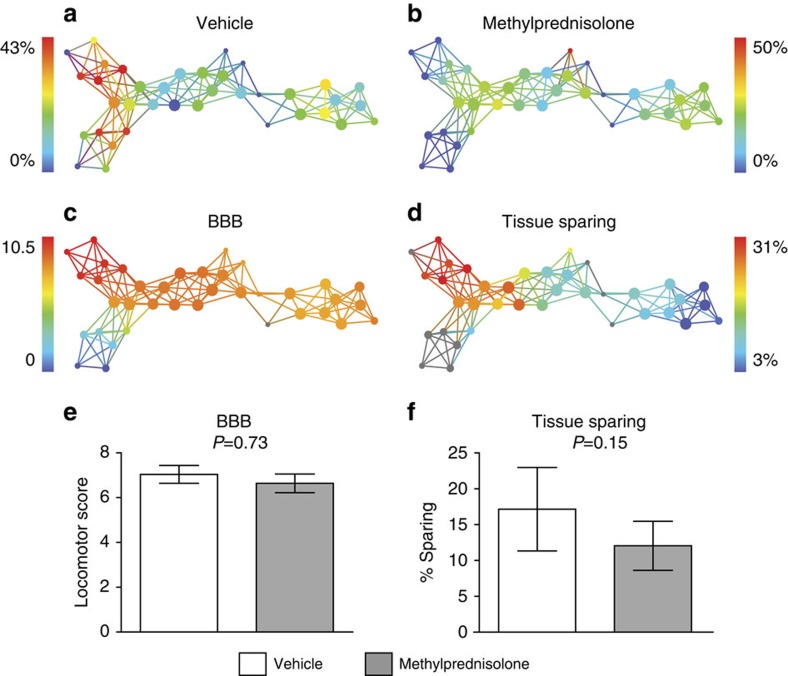
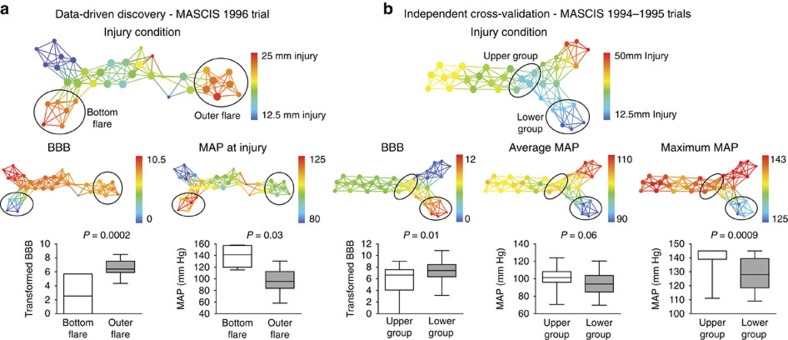
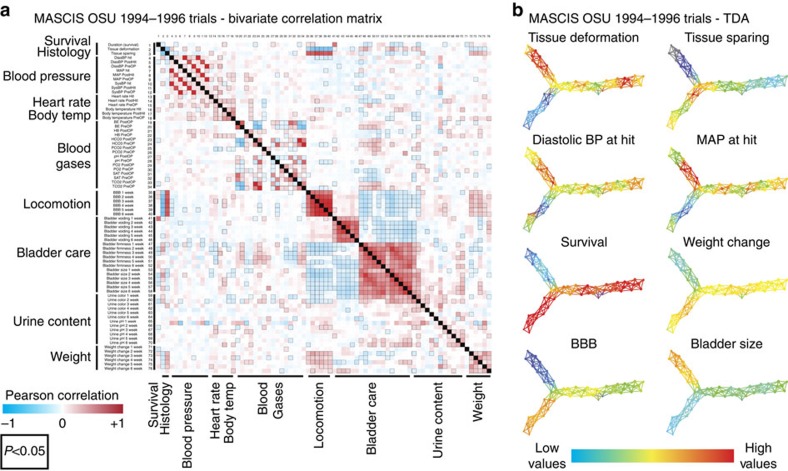
Data-driven discovery in complex neurological disorders has potential to extract meaningful syndromic knowledge from large, heterogeneous data sets to enhance potential for precision medicine. Here we describe the application of topological data analysis (TDA) for data-driven discovery in preclinical traumatic brain injury (TBI) and spinal cord injury (SCI) data sets mined from the Visualized Syndromic Information and Outcomes for Neurotrauma-SCI (VISION-SCI) repository. Through direct visualization of inter-related histopathological, functional and health outcomes, TDA detected novel patterns across the syndromic network, uncovering interactions between SCI and co-occurring TBI, as well as detrimental drug effects in unpublished multicentre preclinical drug trial data in SCI. TDA also revealed that perioperative hypertension predicted long-term recovery better than any tested drug after thoracic SCI in rats. TDA-based data-driven discovery has great potential application for decision-support for basic research and clinical problems such as outcome assessment, neurocritical care, treatment planning and rapid, precision-diagnosis.
Conflict of interest statement
J.P., J.K., T.C.P, P.Y.L, and G.E.C. are current or former employees of Ayasdi Inc. and own shares of the company. All other authors declare no competing financial interests.
Figures
References
-
- Larson E. B. Building trust in the power of "big data" research to serve the public good. JAMA 309, 2443–2444 (2013). - PubMed
-
- Fox P. & Hendler J. Changing the equation on scientific data visualization. Science 331, 705–708 (2011). - PubMed
-
- Gough N. R. & Yaffe M. B. Focus issue: conquering the data mountain. Sci. Signal. 4, eg2 (2011). - PubMed
Publication types
MeSH terms
Grants and funding
- R21 AG032518/AG/NIA NIH HHS/United States
- AG032518/AG/NIA NIH HHS/United States
- R01 NS031193/NS/NINDS NIH HHS/United States
- NS067092/NS/NINDS NIH HHS/United States
- NS031193/NS/NINDS NIH HHS/United States
- NS079030/NS/NINDS NIH HHS/United States
- R01 NS067092/NS/NINDS NIH HHS/United States
- R01 NS069537/NS/NINDS NIH HHS/United States
- NS038079/NS/NINDS NIH HHS/United States
- NS069537/NS/NINDS NIH HHS/United States
- R01 NS038079/NS/NINDS NIH HHS/United States
- F32 NS079030/NS/NINDS NIH HHS/United States
- NS032000/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
