

Update on Sclerosing Cholangitis in Critically Ill Patients
- PMID: 26468312
- PMCID: PMC4569200
- DOI: 10.1159/000431031
Update on Sclerosing Cholangitis in Critically Ill Patients
Abstract
Background: ‛Sclerosing cholangitis in critically ill patients' (SC-CIP) is a cholestatic liver disease of unknown etiology and represents the most prevalent form of secondary sclerosing cholangitis.
Methods: This overview is based on a systematic review of the literature searching for 'secondary sclerosing cholangitis', 'SC-CIP', 'cast syndrome', and 'ischemic cholangitis' in the database PubMed.
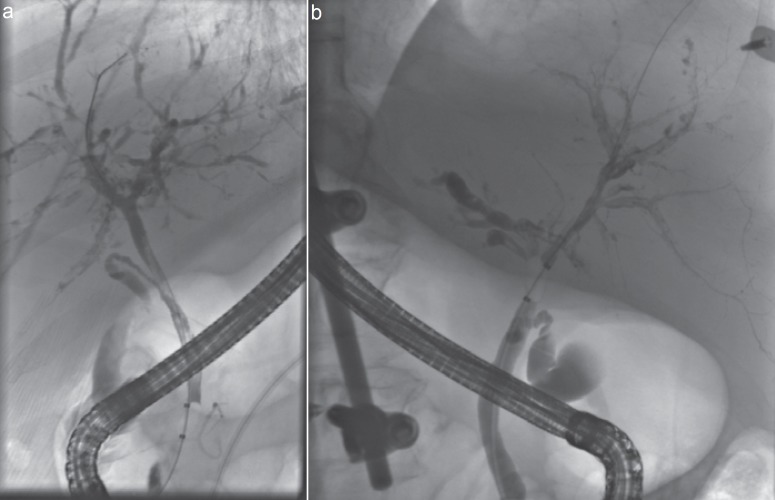
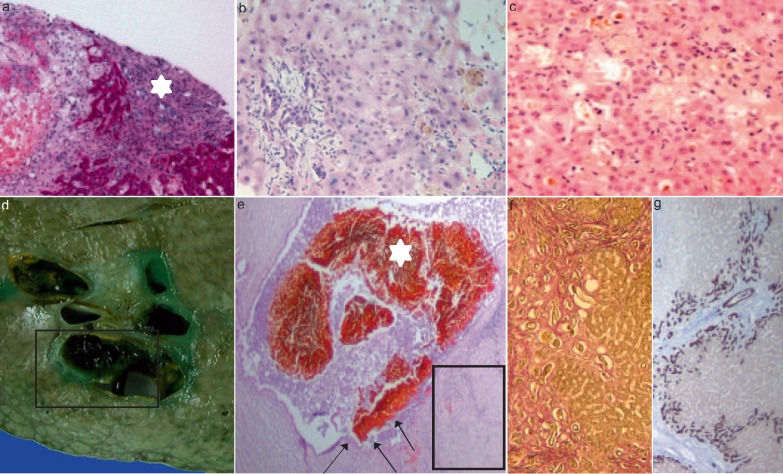
Results: SC-CIP can develop in patients with sepsis and acute respiratory distress syndrome during a long-term intensive care unit (ICU) treatment. It is a rare cholestatic liver disease with a rapid progression to liver cirrhosis and hepatic failure. SC-CIP is initiated by an ischemic injury to the biliary tree with subsequent stenoses of biliary ducts, biliary casts, and infections, often with multi-resistant bacteria. Mechanical ventilation with high positive end-expiratory pressure, prone positioning, and a higher volume of intraperitoneal fat have been proposed as risk factors for developing SC-CIP. Patients with SC-CIP have a poor prognosis, with liver transplantation (LT) being the only curative treatment option.
Conclusion: In patients with sepsis, long-term ICU therapy and ongoing cholestasis SC-CIP must be excluded by endoscopic retrograde cholangiopancreatography. Due to the poor prognosis, the option of LT should be evaluated in all patients with SC-CIP.
Keywords: Cast syndrome; Sclerosing cholangitis in critically ill patients (SC-CIP); Secondary sclerosing cholangitis.
Figures
Similar articles
-
Biliary Cast Syndrome and Secondary Sclerosing Cholangitis in Critically Ill Patient after Long-Term Treatment in the Intensive Care Unit.Case Rep Gastroenterol. 2024 May 10;18(1):260-265. doi: 10.1159/000537957. eCollection 2024 Jan-Dec. Case Rep Gastroenterol. 2024. PMID: 38737441 Free PMC article.
-
Ischemic-like cholangiopathy with secondary sclerosing cholangitis in critically ill patients.Am J Gastroenterol. 2007 Jun;102(6):1221-9. doi: 10.1111/j.1572-0241.2007.01118.x. Am J Gastroenterol. 2007. PMID: 17531010
-
Outcome of patients with ischemic-like cholangiopathy with secondary sclerosing cholangitis after liver transplantation.Scand J Gastroenterol. 2011 Apr;46(4):471-8. doi: 10.3109/00365521.2010.537683. Epub 2010 Nov 30. Scand J Gastroenterol. 2011. PMID: 21114429
-
Secondary sclerosing cholangitis in critically ill patients: current perspectives.Clin Exp Gastroenterol. 2017 Jun 23;10:105-111. doi: 10.2147/CEG.S115518. eCollection 2017. Clin Exp Gastroenterol. 2017. PMID: 28694703 Free PMC article. Review.
-
Secondary sclerosing cholangitis after COVID-19 pneumonia: a report of two cases and review of the literature.Clin J Gastroenterol. 2022 Dec;15(6):1124-1129. doi: 10.1007/s12328-022-01687-5. Epub 2022 Aug 11. Clin J Gastroenterol. 2022. PMID: 35953614 Free PMC article. Review.
Cited by
-
High Rate of Gastrointestinal Bleeding in Patients with Secondary Sclerosing Cholangitis in Critically Ill Patients (SC-CIP).J Clin Med. 2021 Apr 29;10(9):1925. doi: 10.3390/jcm10091925. J Clin Med. 2021. PMID: 33946877 Free PMC article.
-
[Weaning in a Pandemic Situation - A Position Paper].Pneumologie. 2021 Feb;75(2):113-121. doi: 10.1055/a-1337-9848. Epub 2020 Dec 22. Pneumologie. 2021. PMID: 33352589 Free PMC article. German.
-
Post-Covid-19 Cholangiopathy-A New Indication for Liver Transplantation: A Case Report.Transplant Proc. 2021 May;53(4):1132-1137. doi: 10.1016/j.transproceed.2021.03.007. Epub 2021 Mar 12. Transplant Proc. 2021. PMID: 33846012 Free PMC article.
-
Secondary sclerosing cholangitis as a complication of severe COVID-19: A case report and review of the literature.Clin Case Rep. 2021 May 24;9(5):e04068. doi: 10.1002/ccr3.4068. eCollection 2021 May. Clin Case Rep. 2021. PMID: 34084492 Free PMC article.
-
The Gut-Liver Axis in Cholestatic Liver Diseases.Nutrients. 2021 Mar 21;13(3):1018. doi: 10.3390/nu13031018. Nutrients. 2021. PMID: 33801133 Free PMC article. Review.
References
-
- Gossard AA, Angulo P, Lindor KD. Secondary sclerosing cholangitis: a comparison to primary sclerosing cholangitis. Am J Gastroenterol. 2005;100:1330–1333. - PubMed
-
- Ruemmele P, Hofstaedter F, Gelbmann CM. Secondary sclerosing cholangitis. Nat Rev Gastroenterol Hepatol. 2009;6:287–295. - PubMed
-
- Nunes G, Blaisdell FW, Margaretten W. Mechanism of hepatic dysfunction following shock and trauma. Arch Surg. 1970;100:546–556. - PubMed
-
- Champion HR, Jones RT, Trump BF, Decker R, Wilson S, Miginski M, Gill W. A clinicopathologic study of hepatic dysfunction following shock. Surg Gynecol Obstet. 1976;142:657–663. - PubMed
-
- Hartley S, Scott AJ, Spence M. Benign postoperative jaundice complicating severe trauma. N Z Med J. 1977;86:174–178. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
