

How to Diagnose Immunoglobulin G4-Associated Cholangitis: The Jack-of-All-Trades in the Biliary Tract
- PMID: 26468313
- PMCID: PMC4569201
- DOI: 10.1159/000431028
How to Diagnose Immunoglobulin G4-Associated Cholangitis: The Jack-of-All-Trades in the Biliary Tract
Abstract
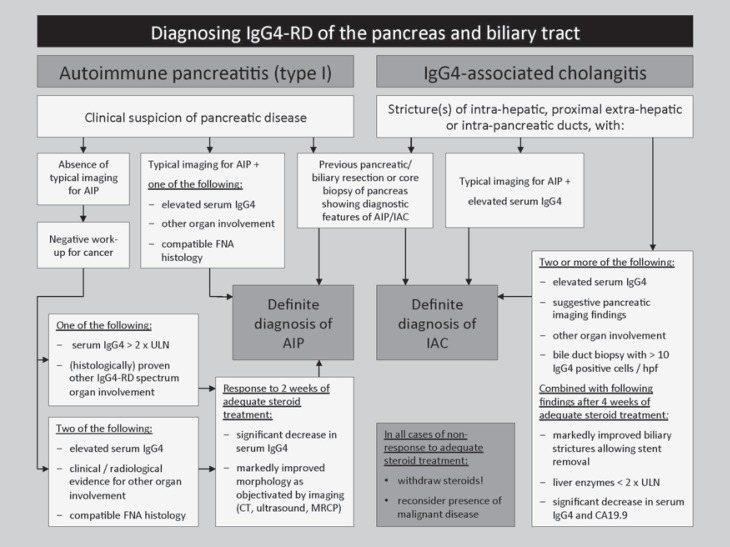
Background: Immunoglobulin (Ig) G4-associated cholangitis (IAC) is an inflammatory disorder of the biliary tract displaying characteristic features of IgG4-related disease (IgG4-RD): elevation of IgG4 serum levels, infiltration of IgG4+ plasma cells in the affected tissue, and good response to immunosuppressive treatment.
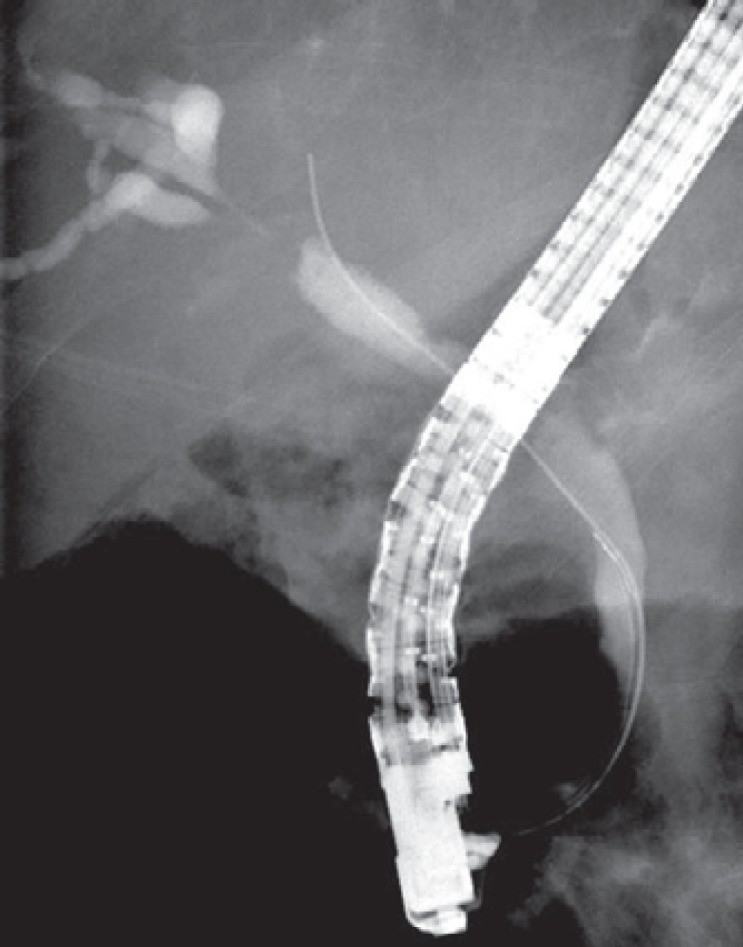
Methods and results: The clinical presentation of IAC is often misleading, mimicking other diseases of the biliary tract such as cholangiocarcinoma or primary and secondary sclerosing cholangitis. The HISORt criteria form the cornerstone in the diagnosis of IAC, combining histopathological (H), imaging (I), and serological (S) features including serum IgG4, other organ manifestations (O) of IgG4-RD and response to treatment (Rt). The accuracy of the HISORt criteria is limited. Novel diagnostic approaches are under evaluation.
Conclusion: More accurate biomarkers are needed to correctly diagnose IgG4-RD and prevent misdiagnoses and unnecessary therapeutic interventions.
Keywords: CCA; Cholangiocarcinoma; IgG4-related systemic disease; PSC; Primary sclerosing cholangitis.
Figures

References
-
- Ghazale A, Chari ST, Zhang L, et al. Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy. Gastroenterology. 2008;134:706–715. - PubMed
-
- Sandanayake NS, Church NI, Chapman MH, et al. Presentation and management of post-treatment relapse in autoimmune pancreatitis/immunoglobulin G4-associated cholangitis. Clin Gastroenterol Hepatol. 2009;7:1089–1096. - PubMed
-
- Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2014;6736:1–12. - PubMed
-
- Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25:1181–1192. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
