

Short-Term Outcomes of Laparoscopic Total Gastrectomy Performed by a Single Surgeon Experienced in Open Gastrectomy: Review of Initial Experience
- PMID: 26468413
- PMCID: PMC4604330
- DOI: 10.5230/jgc.2015.15.3.159
Short-Term Outcomes of Laparoscopic Total Gastrectomy Performed by a Single Surgeon Experienced in Open Gastrectomy: Review of Initial Experience
Abstract
Purpose: Laparoscopic total gastrectomy (LTG) is more complicated than laparoscopic distal gastrectomy, especially during a surgeon's initial experience with the technique. In this study, we evaluated the short-term outcomes of and learning curve for LTG during the initial cases of a single surgeon compared with those of open total gastrectomy (OTG).
Materials and methods: Between 2009 and 2013, 134 OTG and 74 LTG procedures were performed by a single surgeon who was experienced with OTG but new to performing LTG. Clinical characteristics, operative parameters, and short-term postoperative outcomes were compared between groups.
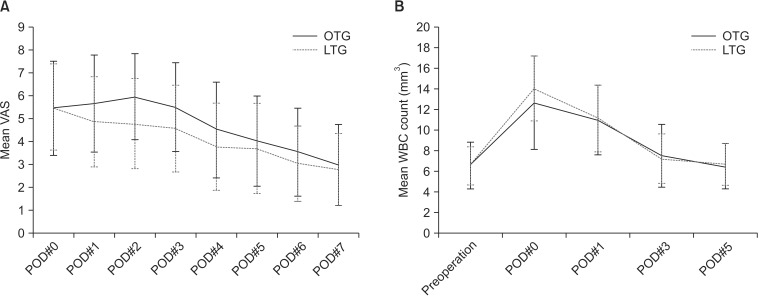
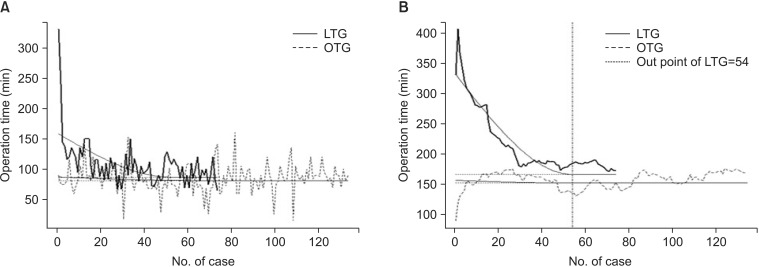
Results: Advanced gastric cancer and D2 lymph node dissection were more common in the OTG than LTG group. Although the operation time was significantly longer for LTG than for OTG (175.7±43.1 minutes vs. 217.5±63.4 minutes), LTG seems to be slightly superior or similar to OTG in terms of postoperative recovery measures. The operation time moving average of 15 cases in the LTG group decreased gradually, and the curve flattened at 54 cases. The postoperative complication rate was similar for the two groups (11.9% vs. 13.5%). No anastomotic or stump leaks occurred.
Conclusions: Although LTG is technically difficult and operation time is longer for surgeons experienced in open surgery, it can be performed safely, even during a surgeon's early experience with the technique. Considering the benefits of minimally invasive surgery, LTG is recommended for early gastric cancer.
Keywords: Laparoscopy; Learning curve; Stomach neoplasms; Total gastrectomy.
Conflict of interest statement
Figures
Comment in
-
Letter to the Editor Concerning "Short-Term Outcomes of Laparoscopic Total Gastrectomy Performed by a Single Surgeon Experienced in Open Gastrectomy: Review of Initial Experience".J Gastric Cancer. 2016 Jun;16(2):125-7. doi: 10.5230/jgc.2016.16.2.125. Epub 2016 Jun 24. J Gastric Cancer. 2016. PMID: 27430723 Free PMC article. No abstract available.
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Chua YJ, Cunningham D. The UK NCRI MAGIC trial of perioperative chemotherapy in resectable gastric cancer: implications for clinical practice. Ann Surg Oncol. 2007;14:2687–2690. - PubMed
-
- Nakajima T. Gastric cancer treatment guidelines in Japan. Gastric Cancer. 2002;5:1–5. - PubMed
-
- Bang YJ, Kim YW, Yang HK, Chung HC, Park YK, Lee KH, et al. CLASSIC trial investigators. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet. 2012;379:315–321. - PubMed
-
- Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010;11:439–449. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
