

Clinical Outcome of Modified Laparoscopy-Assisted Proximal Gastrectomy Compared to Conventional Proximal Gastrectomy or Total Gastrectomy for Upper-Third Early Gastric Cancer with Special References to Postoperative Reflux Esophagitis
- PMID: 26468417
- PMCID: PMC4604334
- DOI: 10.5230/jgc.2015.15.3.191
Clinical Outcome of Modified Laparoscopy-Assisted Proximal Gastrectomy Compared to Conventional Proximal Gastrectomy or Total Gastrectomy for Upper-Third Early Gastric Cancer with Special References to Postoperative Reflux Esophagitis
Abstract
Purpose: This study evaluated the functional and oncological outcomes of proximal gastrectomy (PG) in comparison with total gastrectomy (TG) for upper-third early gastric cancer (EGC).
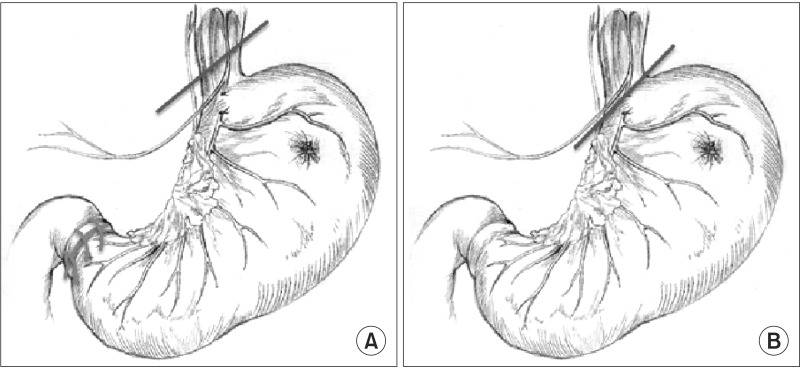
Materials and methods: The medical records of upper-third EGC patients who had undergone PG (n=192) or TG (n=157) were reviewed. The PG group was further subdivided into patients who had undergone conventional open PG (cPG; n=157) or modified laparoscopy-assisted PG (mLAPG; n=35). Patients who had undergone mLAPG had a longer portion of their intra-abdominal esophagus preserved than patients who had undergone cPG. Surgical morbidity, recurrence, long-term nutritional status, and the incidence of reflux esophagitis were compared between the groups.
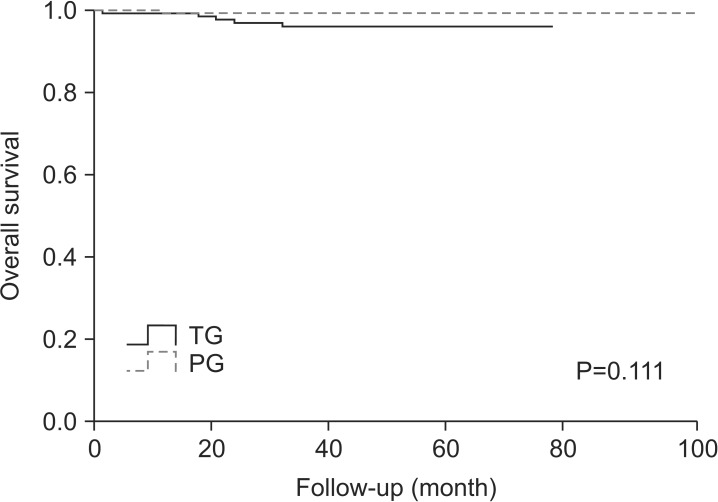
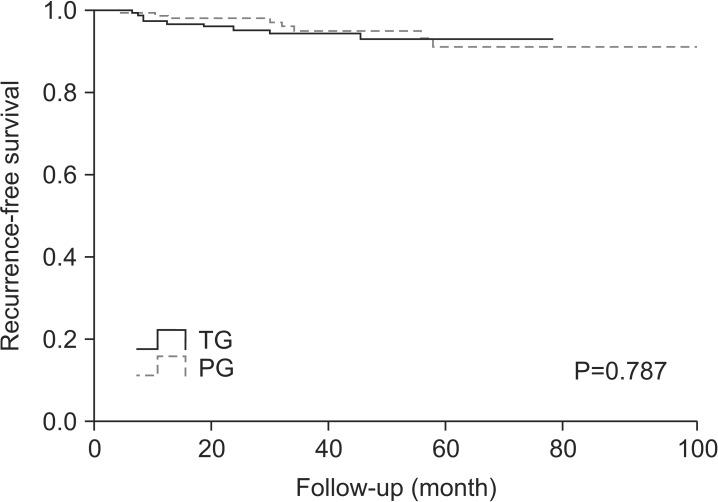
Results: The rate of postoperative complications was significantly lower for PG than TG (16.7% vs. 31.2%), but the five-year overall survival rate was comparable between the two groups (99.3% vs. 96.3%). Postoperative levels of hemoglobin and albumin were significantly higher for patients who had undergone PG. However, the incidence of reflux esophagitis was higher for PG than for TG (37.4% vs. 3.7%; P<0.001). mLAPG was related to a lower incidence of reflux esophagitis after PG (P<0.001).
Conclusions: Compared to TG, PG showed an advantage in terms of postoperative morbidity and nutrition, and there was a comparable prognosis between the two procedures. Preserving the intra-abdominal esophagus may lower the incidence of reflux esophagitis associated with PG.
Keywords: Gastrectomy; Laparoscopy; Stomach neoplasms.
Conflict of interest statement
Figures
References
-
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3) Gastric Cancer. 2011;14:113–123. - PubMed
-
- Harrison LE, Karpeh MS, Brennan MF. Total gastrectomy is not necessary for proximal gastric cancer. Surgery. 1998;123:127–130. - PubMed
-
- Katsoulis IE, Robotis JF, Kouraklis G, Yannopoulos PA. What is the difference between proximal and total gastrectomy regarding postoperative bile reflux into the oesophagus? Dig Surg. 2006;23:325–330. - PubMed
-
- Ahn HS, Lee HJ, Yoo MW, Jeong SH, Park DJ, Kim HH, et al. Changes in clinicopathological features and survival after gastrectomy for gastric cancer over a 20-year period. Br J Surg. 2011;98:255–260. - PubMed
-
- Hirai T, Matsumoto H, Iki K, Hirabayashi Y, Kawabe Y, Ikeda M, et al. Lower esophageal sphincter- and vagus-preserving proximal partial gastrectomy for early cancer of the gastric cardia. Surg Today. 2006;36:874–878. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
