

Basal ganglia T1 hyperintensity in LGI1-autoantibody faciobrachial dystonic seizures
- PMID: 26468474
- PMCID: PMC4592539
- DOI: 10.1212/NXI.0000000000000161
Basal ganglia T1 hyperintensity in LGI1-autoantibody faciobrachial dystonic seizures
Abstract
Objective: To characterize the clinical features and MRI abnormalities of leucine-rich glioma-inactivated 1 (LGI1)-autoantibody (Ab) faciobrachial dystonic seizures (FBDS).
Methods: Forty-eight patients with LGI1-Ab encephalopathy were retrospectively identified by searching our clinical and serologic database from January 1, 2002, to June 1, 2015. Of these, 26 met inclusion criteria for this case series: LGI1-Ab seropositivity and FBDS. In a separate analysis of all 48 patients initially identified, the MRIs of patients with (n = 26) and without (n = 22) FBDS were compared by 2 neuroradiologists blinded to the clinical details.
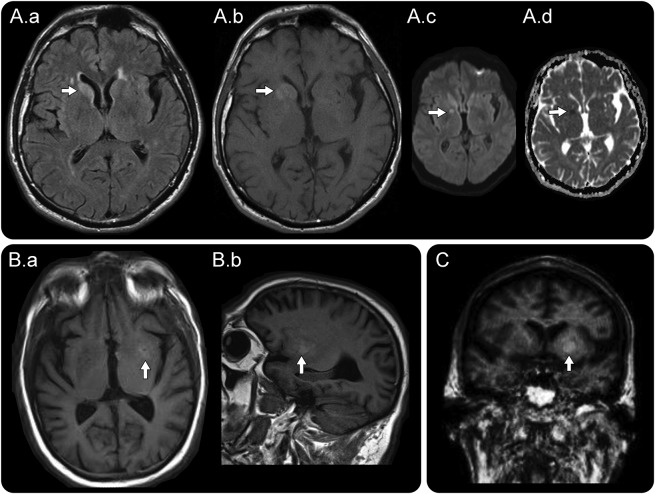
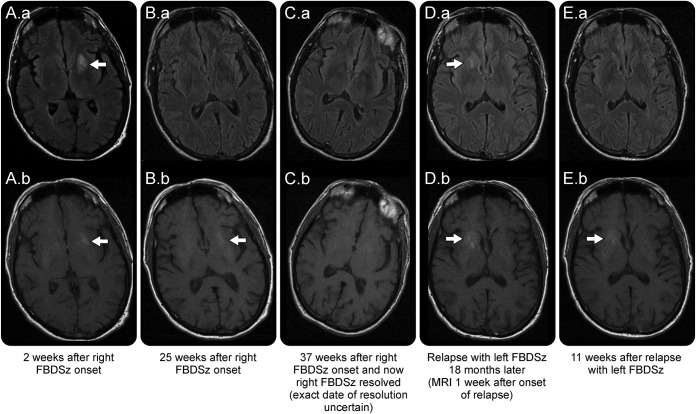
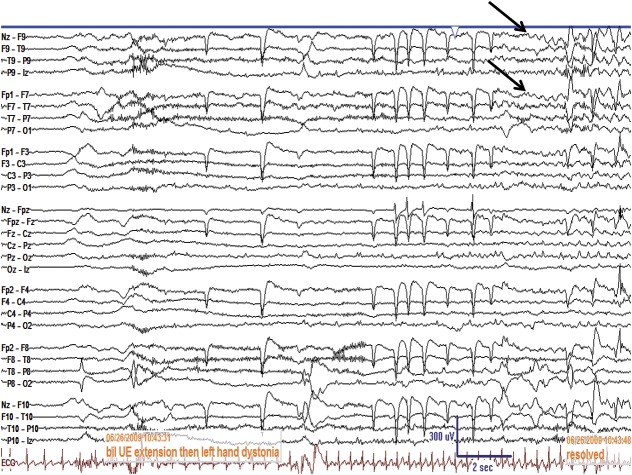
Results: The median age of the 26 included patients was 62.5 years (range 37-78); 65% were men. FBDS involved arm (26), face (22), and leg (12). Ten were previously diagnosed as psychogenic. Ictal EEGs were normal in 20 of 23 assessed. Basal ganglia T1 and T2 signal abnormalities were detected in 11 patients (42%), with excellent agreement between neuroradiologists (κ scores of 0.86 and 0.93, respectively), and included T1 hyperintensity alone (2), T2 hyperintensity alone (1), or both (8). The T1 hyperintensities persisted longer than the T2 hyperintensities (median 11 weeks vs 1 week, p = 0.02). Improvement with immunotherapy (18/18) was more frequent than with antiepileptic medications (10/24). A separate analysis of all 48 patients initially identified with LGI1-Ab encephalopathy showed that basal ganglia MRI abnormalities were present in 11 of 26 with FBDS but not present in those without FBDS (0/22) (p < 0.001). In contrast, mesial temporal MRI abnormalities were less common among those with FBDS (42%) than those without (91%) (p < 0.001).
Conclusions: Basal ganglia T1 hyperintensity is a clinically useful MRI biomarker of LGI1-Ab FBDS and suggests a basal ganglia localization.
Figures
References
-
- Irani SR, Buckley C, Vincent A, et al. Immunotherapy-responsive seizure-like episodes with potassium channel antibodies. Neurology 2008;71:1647–1648. - PubMed
-
- Irani SR, Michell AW, Lang B, et al. Faciobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis. Ann Neurol 2011;69:892–900. - PubMed
-
- Irani SR, Stagg CJ, Schott JM, et al. Faciobrachial dystonic seizures: the influence of immunotherapy on seizure control and prevention of cognitive impairment in a broadening phenotype. Brain 2013;136:3151–3162. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous