

Review
doi: 10.1038/nature15817.
Pharmacogenomics in the clinic
Affiliations
- PMID: 26469045
- PMCID: PMC4711261
- DOI: 10.1038/nature15817
Item in Clipboard
Review
Pharmacogenomics in the clinic
Nature.
.
Abstract
After decades of discovery, inherited variations have been identified in approximately 20 genes that affect about 80 medications and are actionable in the clinic. And some somatically acquired genetic variants direct the choice of 'targeted' anticancer drugs for individual patients. Current efforts that focus on the processes required to appropriately act on pharmacogenomic variability in the clinic are moving away from discovery and towards implementation of an evidenced-based strategy for improving the use of medications, thereby providing a cornerstone for precision medicine.
Figures
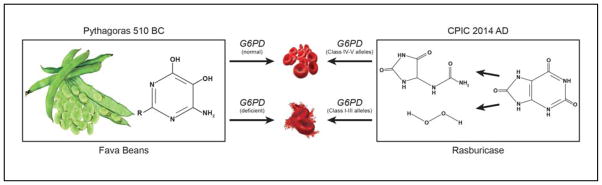
Pythagoras is thought to have banned the consumption of fava beans (vicia fava) after observing that their ingestion caused hemolytic anemia in a subset of people (left). This was subsequently shown to occur predominantly in persons with glucose-6-phosphate dehydrogenase (G6PD) deficiency, primarily persons who inherited the Class II “Mediterranean allele” of G6PD. The chemical moieties in fava beans thought to cause hemolysis in G6PD-deficient individuals are isouramil (R=OH) and divicine (R=NH2), pyrimidine aglycones of two glucosides found in fava beans. (vicine and convicine). Multiple medications also cause oxidative stress and erythrocytes of G6PD deficient individuals produce insufficient NADPH to protect from oxidative damage, and hemolysis and methemoglobinemia can ensue. Rasburicase is a recombinant form of urate oxidase that is used clinically to lower uric acid levels in the treatment of tumor lysis syndrome (right). The oxidative stress caused by hydrogen peroxide produced when rasburicase cleaves uric acid to allantoin and hydroperoxide is more likely to cause hemolytic anemia and methemoglobinemia in persons who have inherited G6PD deficiency; rasburicase is contraindicated in G6PD deficient individuals.
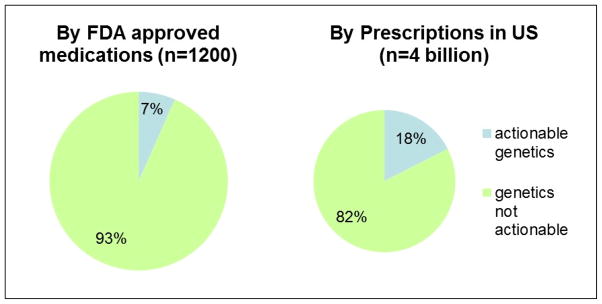
Approximately 7% percentage of medications (FDA approved) are affected by actionable inherited pharmacogenes (right), whereas approximately 18% of outpatient prescriptions in the US are affected by actionable germline pharmacogenomics (left), illustrating that several pharmacogenetically high-risk drugs are commonly prescribed.
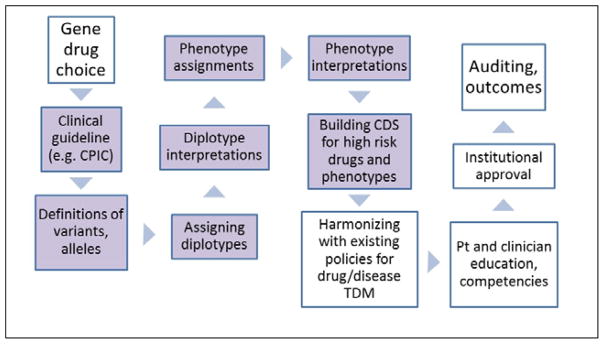
Multiple steps in bringing pharmacogenomic tests to the clinic. These include prioritizing the choice of gene(s)/drug(s) for actionability; CPIC guidelines exist or are being developed for all actionable inherited pharmacogenes, and the guidelines provide guidance for the steps shaded in lavender. Genotypes must be assigned to alleles, and diplotypes assigned to patients. The diplotypes must be translated into phenotypes (gene function) and interpreted with respect to drug therapy. Appropriate clinical decision support (CDS) should be built and deployed to provide prescribers with recommendations, and pharmacogenetic considerations must be harmonized with other policies for the affected medications, using therapeutic drug monitoring (TDM) where applicable. Education of clinicians and of patients should take place, and institutional oversight committees may approve prescribing recommendations and policies. Many groups are auditing clinical and prescribing outcomes to evaluate the impact of clinical implementation of pharmacogenomics.
References
-
- Hughes D, Andersson DI. Evolutionary consequences of drug resistance: shared principles across diverse targets and organisms. Nat Rev Genet. 2015;16(8):459–471. - PubMed
-
- Evans WE, Relling MV. Moving towards individualized medicine with pharmacogenomics. Nature. 2004;429(6990):464–468. Review of pharmacogenomics from discovery to the clinic. - PubMed
-
- Alving AS, Carson PE, Flanagan CL, Ickes CE. Enzymatic deficiency in primaquine-sensitive erythrocytes. Science. 1956;124(3220):484–485. - PubMed
-
- Motulsky AG. Drug reactions enzymes, and biochemical genetics. J Am Med Assoc. 1957;165(7):835–837. - PubMed
-
- Kalow W, Genest K. A method for the detection of atypical forms of human serum cholinesterase; determination of dibucaine numbers. Can J Biochem Physiol. 1957;35(6):339–346. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
