

Time-Limited Trials of Intensive Care for Critically Ill Patients With Cancer: How Long Is Long Enough?
- PMID: 26469222
- PMCID: PMC4713248
- DOI: 10.1001/jamaoncol.2015.3336
Time-Limited Trials of Intensive Care for Critically Ill Patients With Cancer: How Long Is Long Enough?
Abstract
Importance: Time-limited trials of intensive care are commonly used in patients perceived to have a poor prognosis. The optimal duration of such trials is unknown. Factors such as a cancer diagnosis are associated with clinician pessimism and may affect the decision to limit care independent of a patient's severity of illness.
Objective: To identify the optimal duration of intensive care for short-term mortality in critically ill patients with cancer.
Design, setting, and participants: Decision analysis using a state-transition microsimulation model was performed to simulate the hospital course of patients with poor-prognosis primary tumors, metastatic disease, or hematologic malignant neoplasms admitted to medical and surgical intensive care units. Transition probabilities were derived from 920 participants stratified by sequential organ failure assessment (SOFA) scores to identify severity of illness. The model was validated in 3 independent cohorts with 349, 158, and 117 participants from quaternary care academic hospitals. Monte Carlo microsimulation was performed, followed by probabilistic sensitivity analysis. Outcomes were assessed in the overall cohort and in solid tumors alone.
Interventions: Time-unlimited vs time-limited trials of intensive care.
Main outcomes and measures: 30-day all-cause mortality and mean survival duration.
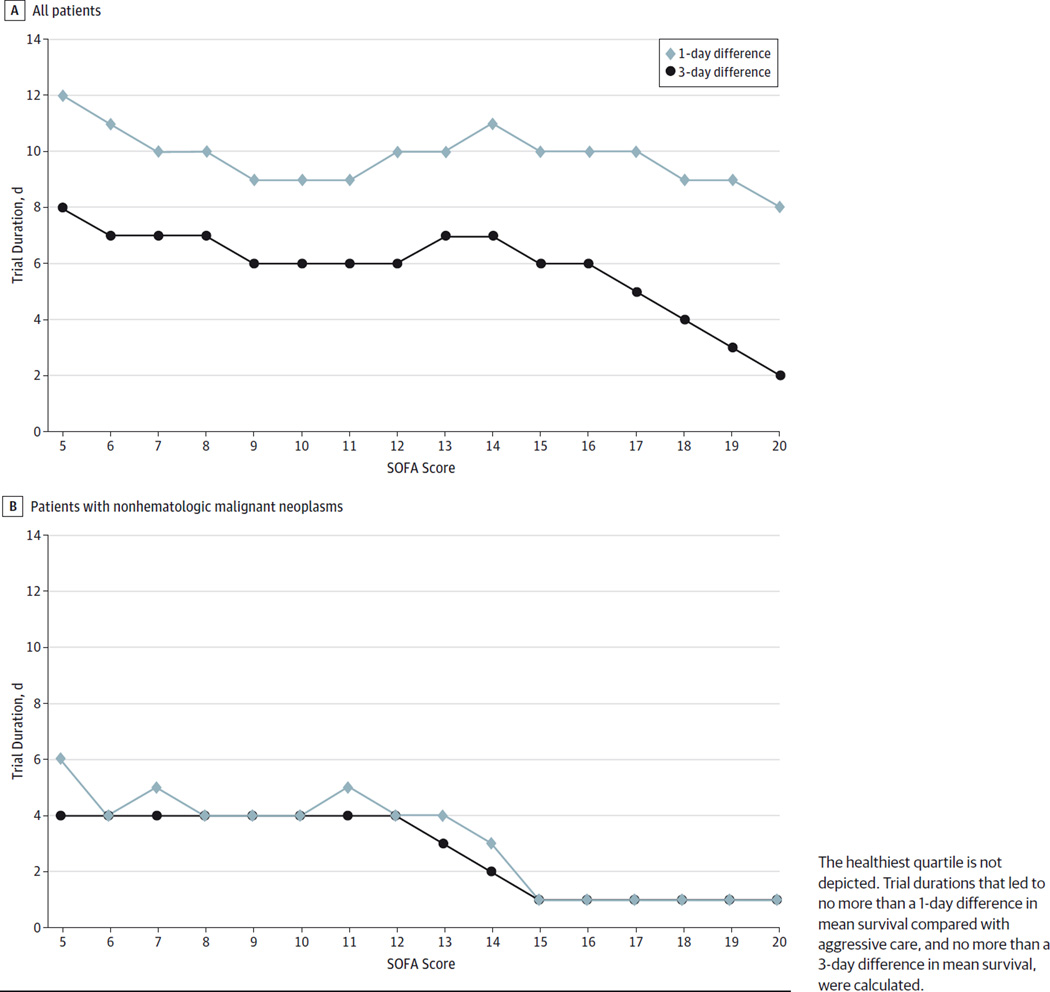
Results: The SOFA scores at ICU admission were significantly associated with mortality. A 3-, 8-, or 15-day trial of intensive care resulted in decreased mean 30-day survival vs aggressive care in all but the sickest patients (SOFA score, 5-9: 48.4% [95% CI, 48.0%-48.8%], 60.6% [95% CI, 60.2%-61.1%], and 66.8% [95% CI, 66.4%-67.2%], respectively, vs 74.6% [95% CI, 74.3%-75.0%] with time-unlimited aggressive care; SOFA score, 10-14: 36.2% [95% CI, 35.8%-36.6%], 44.1% [95% CI, 43.6%-44.5%], and 46.1% [95% CI, 45.6%-46.5%], respectively, vs 48.4% [95% CI, 48.0%-48.8%] with aggressive care; SOFA score, ≥ 15: 5.8% [95% CI, 5.6%-6.0%], 8.1% [95% CI, 7.9%-8.3%], and 8.3% [95% CI, 8.1%-8.6%], respectively, vs 8.8% [95% CI, 8.5%-9.0%] with aggressive care). However, the clinical magnitude of these differences was variable. Trial durations of 8 days in the sickest patients offered mean survival duration that was no more than 1 day different from time-unlimited care, whereas trial durations of 10 to 12 days were required in healthier patients. For the subset of patients with solid tumors, trial durations of 1 to 4 days offered mean survival that was not statistically significantly different from time-unlimited care.
Conclusions and relevance: Trials of ICU care lasting 1 to 4 days may be sufficient in patients with poor-prognosis solid tumors, whereas patients with hematologic malignant neoplasms or less severe illness seem to benefit from longer trials of intensive care.
Conflict of interest statement
No other disclosures are reported.
Figures
Comment in
-
Critically Ill Patients' Preferences Regarding Aggressive Medical Interventions: Can We Hear the Patient's Voice?JAMA Oncol. 2016 Jan;2(1):83-4. doi: 10.1001/jamaoncol.2015.3613. JAMA Oncol. 2016. PMID: 26468919 No abstract available.
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32(3):638–643. - PubMed
-
- Christakis NA, Iwashyna TJ. Attitude and self-reported practice regarding prognostication in a national sample of internists. Arch Intern Med. 1998;158(21):2389–2395. - PubMed
-
- Sinuff T, Adhikari NK, Cook DJ, et al. Mortality predictions in the intensive care unit: comparing physicians with scoring systems. Crit Care Med. 2006;34(3):878–885. - PubMed
-
- Meadow W, Pohlman A, Frain L, et al. Power and limitations of daily prognostications of death in the medical intensive care unit. Crit Care Med. 2011;39(3):474–479. - PubMed
-
- Meadow W, Pohlman A, Reynolds D, et al. Power and limitations of daily prognostications of death in the medical ICU for outcomes in the following 6 months. Crit Care Med. 2014;42(11):2387–2392. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
