

Clinical Characteristics and Outcomes for Solitary Fibrous Tumor (SFT): A Single Center Experience
- PMID: 26469269
- PMCID: PMC4607370
- DOI: 10.1371/journal.pone.0140362
Clinical Characteristics and Outcomes for Solitary Fibrous Tumor (SFT): A Single Center Experience
Abstract
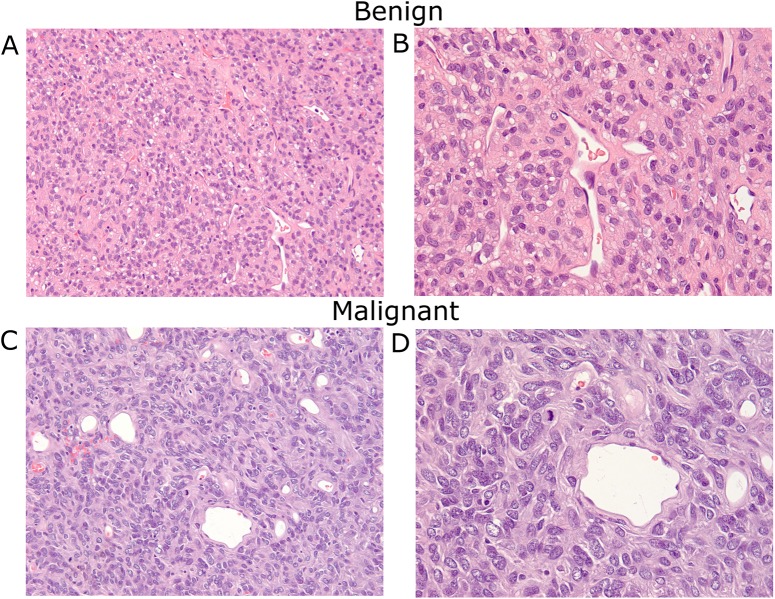
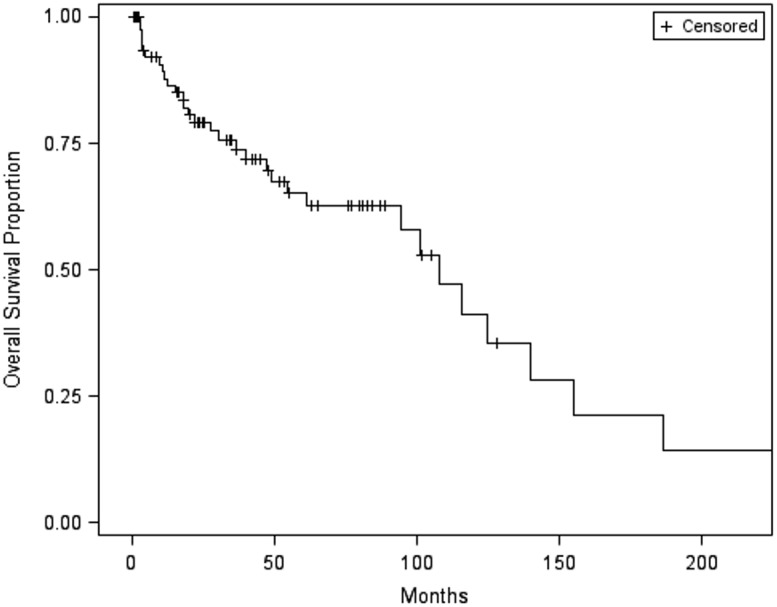
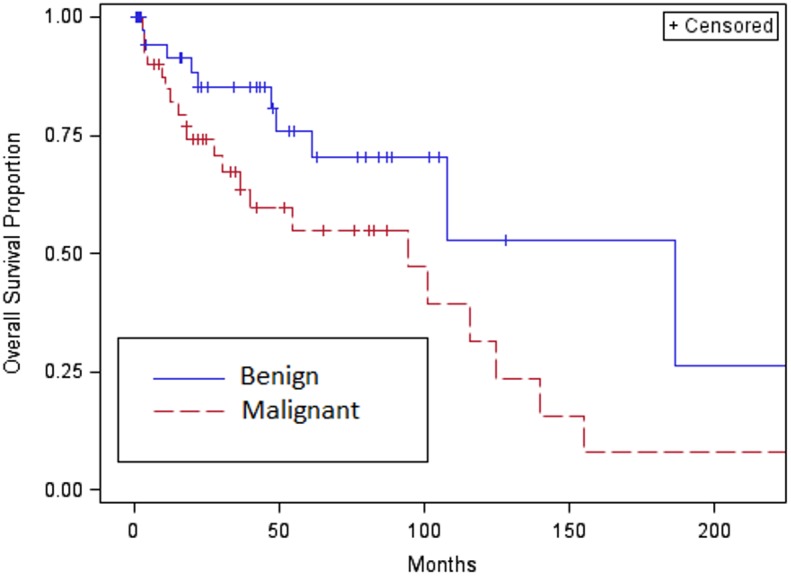
Solitary fibrous tumor (SFT) is a mesenchymal neoplasm of fibrous origin. The 2013 WHO classification of soft tissue tumors defines malignant forms as hypercellular, mitotically active (>4 mitosis/10 high-power fields), with cytological atypia, tumor necrosis, and/or infiltrative margins. With an IRB-approved protocol, we investigated patient records and clinicopathologic data from our Sarcoma Database to describe the clinical characteristics of both benign and malignant SFT. All pathology specimens were reviewed by two pathologists. Descriptive statistics and univariate/multivariate survival analysis were performed. Patient records and Social Security Death Index were used to evaluate vital status. Of 82 patients, 47 (57%) were women and 73 (89%) were Caucasian. Median age was 62 years (range, 20 to 89). Thirty-two (39%) patients succumbed to the disease. Primary tumor site was lung/pleura in 28 (34%), abdomen/pelvis in 23 (28%), extremity in 13 (16%), and head/neck in 9 (11%) patients. Pathology was described as benign in 42 (51%) and malignant in 40 (49%) patients. Compared to benign SFT, malignant histology is associated with larger tumor size, higher mitotic counts, metastatic disease at diagnosis, and greater use of chemotherapy and radiation therapy. Gender, age, and tumor site were not significantly different between benign and malignant subtypes. By univariate analysis, only benign vs. malignant variant and complete resection positively impacted overall survival (P = 0.02 and P<0.0001, respectively). In the multivariable analysis of overall survival, receiving chemotherapy or not receiving surgery were two variables significantly associated with higher failure rate in overall survival: patients with chemotherapy vs. no chemotherapy (P = 0.003, HR = 4.55, with 95% CI: 1.68-12.34) and patients without surgery vs. with surgery (P = 0.005, HR = 25.49, with 95% CI: 2.62-247.57). Clear survival differences exist between benign and malignant SFT. While surgery appears to be the best treatment option for benign and malignant SFT, better systemic therapies are needed to improve outcomes of patients with metastatic, malignant SFT.
Conflict of interest statement
Figures
References
-
- Fletcher C DM., Bridge JA, Lee JC Extrapleural solitary fibrous tumor World Health Organization Classification of Tumours of Soft Tissue and Bone. Lyon, France: IARC Press; 2013; 81.
-
- Gengler C, Guillou L. Solitary fibrous tumour and haemangiopericytoma: evolution of a concept. Histopathology. 2006;48:63–74. - PubMed
-
- Enzinger FM, Smith BH. Hemangiopericytoma. An analysis of 106 cases. Hum Pathol. 1976;7:61–82. - PubMed
-
- Mena H, Ribas JL, Pezeshkpour GH, Cowan DN, Parisi JE. Hemangiopericytoma of the central nervous system: a review of 94 cases. Hum Pathol. 1991;22:84–91. - PubMed
-
- Park MS, Araujo DM. New insights into the hemangiopericytoma/solitary fibrous tumor spectrum of tumors. Curr Opin Oncol. 2009;21:327–331. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
