

Use of Mesh in Laparoscopic Paraesophageal Hernia Repair: A Meta-Analysis and Risk-Benefit Analysis
- PMID: 26469286
- PMCID: PMC4607492
- DOI: 10.1371/journal.pone.0139547
Use of Mesh in Laparoscopic Paraesophageal Hernia Repair: A Meta-Analysis and Risk-Benefit Analysis
Erratum in
-
Correction: Use of Mesh in Laparoscopic Paraesophageal Hernia Repair: A Meta-Analysis and Risk-Benefit Analysis.PLoS One. 2017 Feb 3;12(2):e0171865. doi: 10.1371/journal.pone.0171865. eCollection 2017. PLoS One. 2017. PMID: 28158277 Free PMC article.
Abstract
Introduction: Mesh augmentation seems to reduce recurrences following laparoscopic paraesophageal hernia repair (LPHR). However, there is an uncertain risk of mesh-associated complications. Risk-benefit analysis might solve the dilemma.
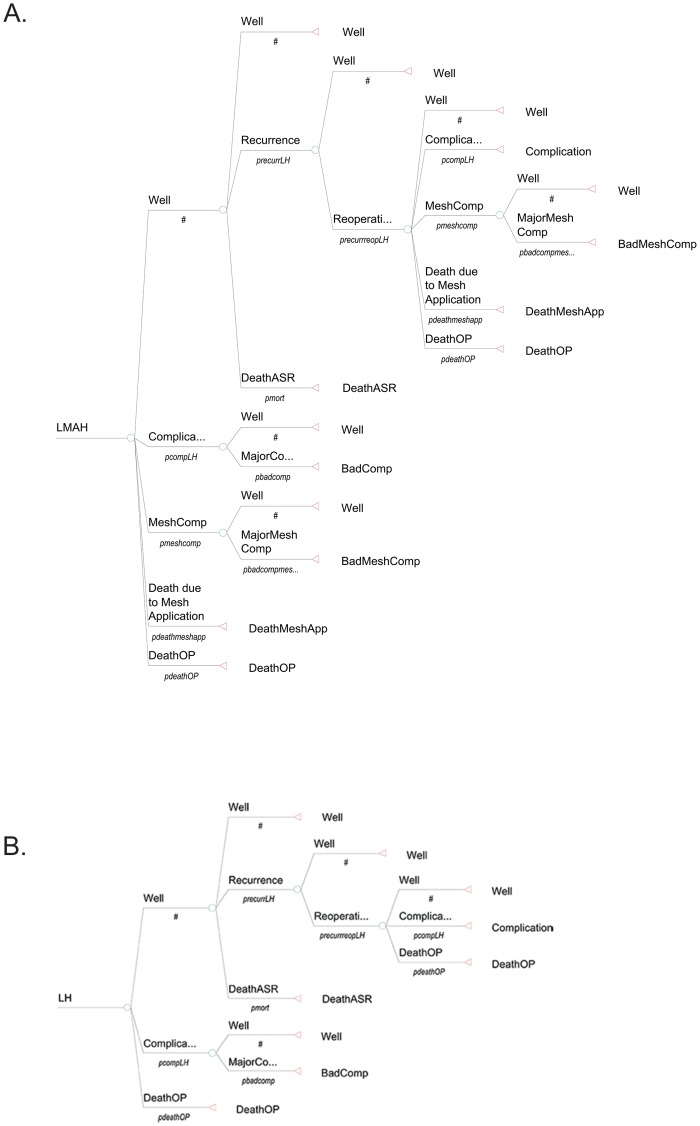
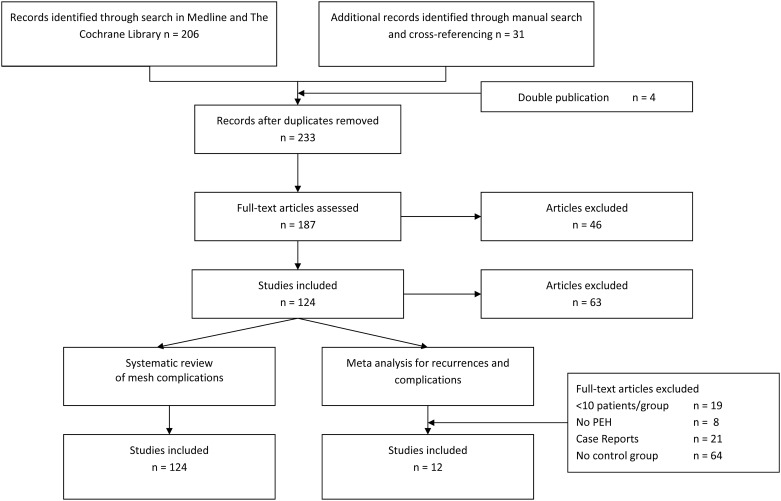
Materials and methods: A systematic literature search was performed to identify randomized controlled trials (RCTs) and observational clinical studies (OCSs) comparing laparoscopic mesh-augmented hiatoplasty (LMAH) with laparoscopic mesh-free hiatoplasty (LH) with regard to recurrences and complications. Random effects meta-analyses were performed to determine potential benefits of LMAH. All data regarding LMAH were used to estimate risk of mesh-associated complications. Risk-benefit analysis was performed using a Markov Monte Carlo decision-analytic model.
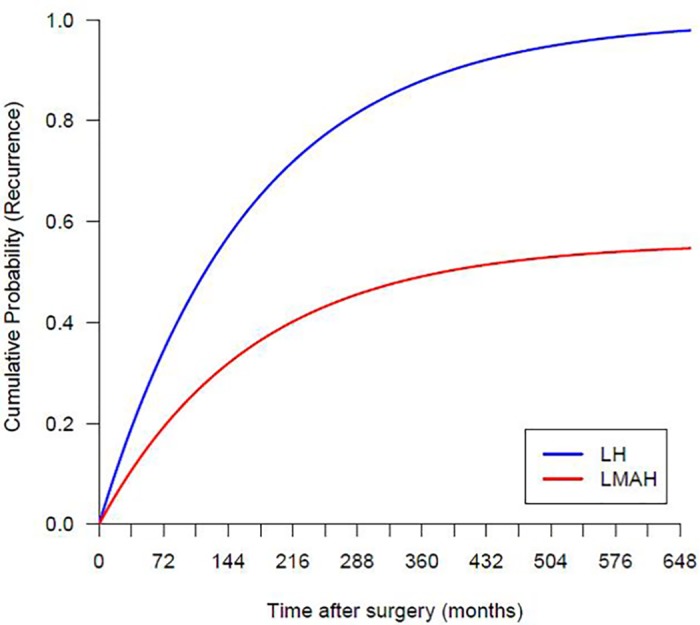
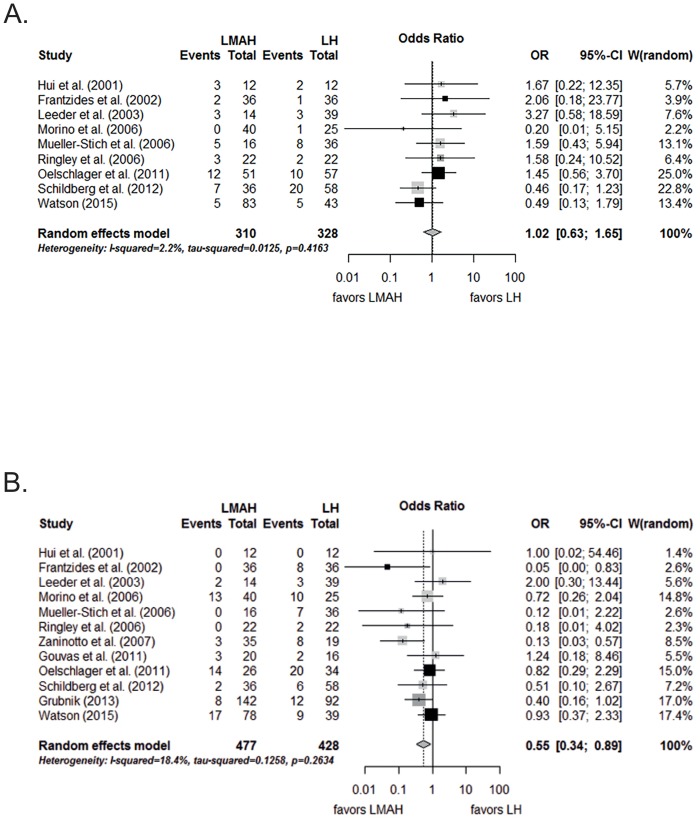
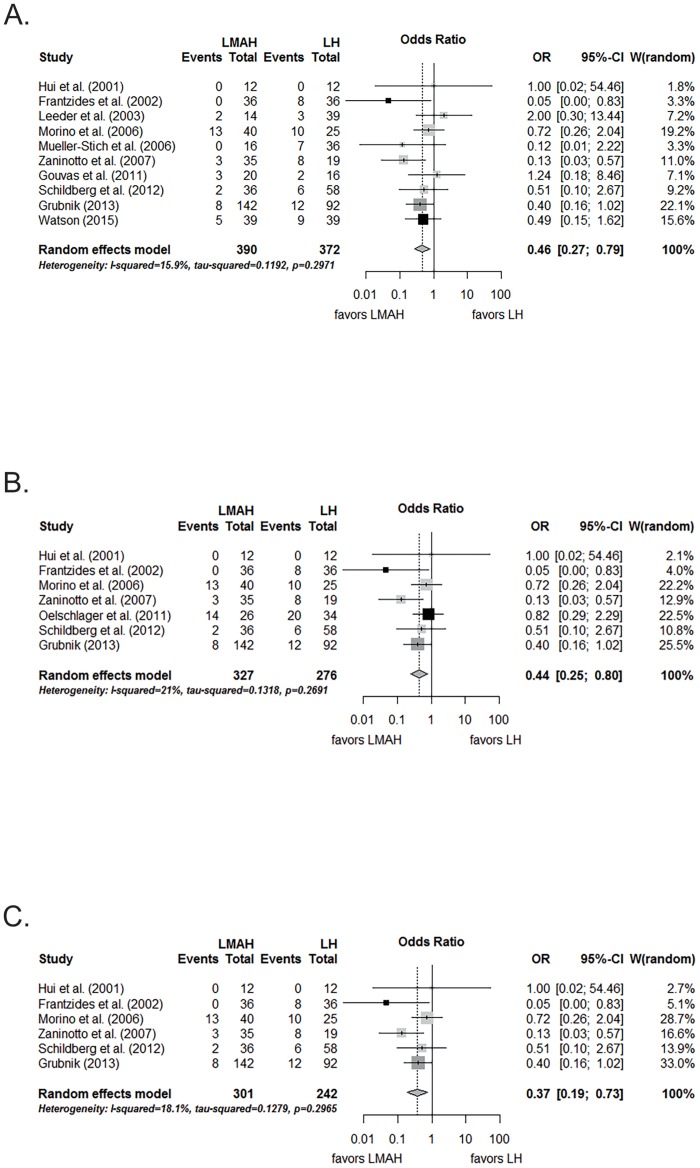
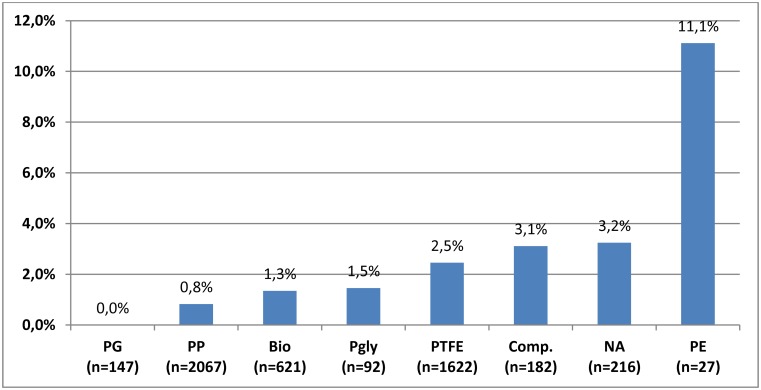
Results: Meta-analysis of 3 RCTs and 9 OCSs including 915 patients revealed a significantly lower recurrence rate for LMAH compared to LH (pooled proportions, 12.1% vs. 20.5%; odds ratio (OR), 0.55; 95% confidence interval (CI), 0.34 to 0.89; p = 0.04). Complication rates were comparable in both groups (pooled proportions, 15.3% vs. 14.2%; OR, 1.02; 95% CI, 0.63 to 1.65; p = 0.94). The systematic review of LMAH data yielded a mesh-associated complication rate of 1.9% (41/2121; 95% CI, 1.3% to 2.5%) for those series reporting at least one mesh-associated complication. The Markov Monte Carlo decision-analytic model revealed a procedure-related mortality rate of 1.6% for LMAH and 1.8% for LH.
Conclusions: Mesh application should be considered for LPHR because it reduces recurrences at least in the mid-term. Overall procedure-related complications and mortality seem to not be increased despite of potential mesh-associated complications.
Conflict of interest statement
Figures
References
-
- Hashemi M, Peters JH, DeMeester TR, Huprich JE, Quek M, Hagen JA, et al. Laparoscopic repair of large type III hiatal hernia: objective followup reveals high recurrence rate. Journal of the American College of Surgeons. 2000;190(5):553–60; discussion 60–1. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
