

Piloting Upfront Xpert MTB/RIF Testing on Various Specimens under Programmatic Conditions for Diagnosis of TB & DR-TB in Paediatric Population
- PMID: 26469691
- PMCID: PMC4607299
- DOI: 10.1371/journal.pone.0140375
Piloting Upfront Xpert MTB/RIF Testing on Various Specimens under Programmatic Conditions for Diagnosis of TB & DR-TB in Paediatric Population
Abstract
Background: India accounts for one-fifth of the global TB incidence. While the exact burden of childhood TB is not known, TB remains one of the leading causes of childhood mortality in India. Bacteriological confirmation of TB in children is challenging due to difficulty in obtaining quality specimens, in the absence of which diagnosis is largely based on clinical judgement. While testing multiple specimens can potentially contribute to higher proportion of laboratory confirmed paediatric TB cases, lack of high sensitivity tests adds to the diagnostic challenge. We describe here our experiences in piloting upfront Xpert MTB/RIF testing, for diagnosis of TB in paediatric population in respiratory and extra pulmonary specimens, as recently recommended by WHO.
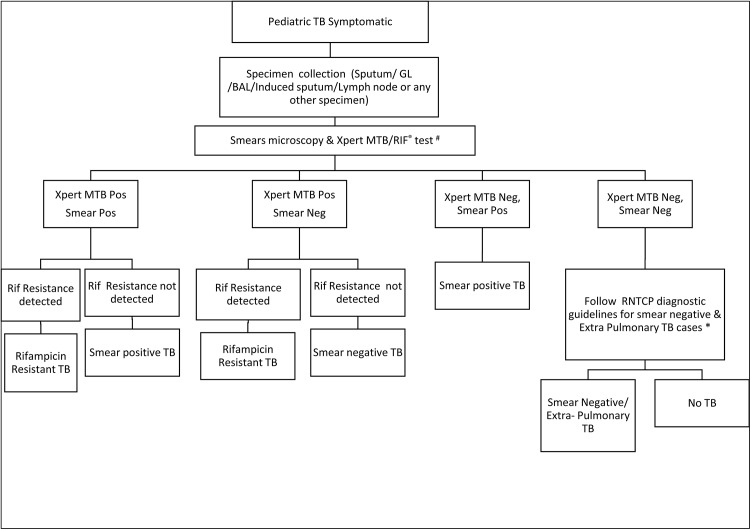
Method: Xpert MTB/RIF testing was offered to all paediatric (0-14 years) presumptive TB cases (both pulmonary and extra-pulmonary) seeking care at public and private health facilities in the project areas covering 4 cities of India.
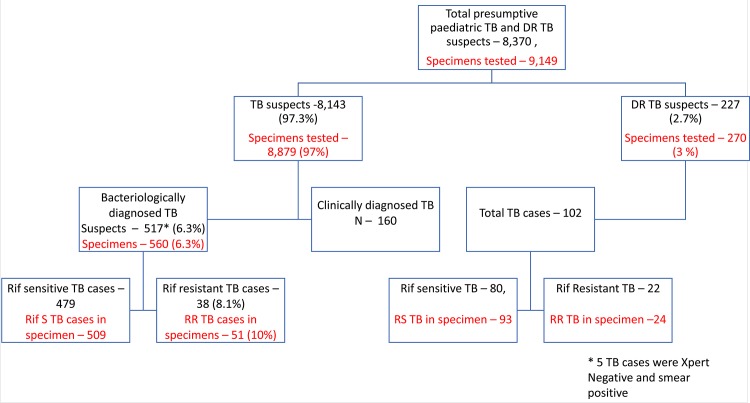
Results: Under this pilot project, 8,370 paediatric presumptive TB & presumptive DR-TB cases were tested between April and-November 2014. Overall, 9,149 specimens were tested, of which 4,445 (48.6%) were non-sputum specimens. Xpert MTB/RIF gave 9,083 (99.2%, CI 99.0-99.4) valid results. Of the 8,143 presumptive TB cases enrolled, 517 (6.3%, CI 5.8-6.9) were bacteriologically confirmed. TB detection rates were two fold higher with Xpert MTB/RIF as compared to smear microscopy. Further, a total of 60 rifampicin resistant TB cases were detected, of which 38 were detected among 512 presumptive TB cases while 22 were detected amongst 227 presumptive DR-TB cases tested under the project.
Conclusion: Xpert MTB/RIF with advantages of quick turnaround testing-time, high proportion of interpretable results and feasibility of rapid rollout, substantially improved the diagnosis of bacteriologically confirmed TB in children, while simultaneously detecting rifampicin resistance.
Conflict of interest statement
Figures

References
-
- Vadwai V, Boehme C, Nabeta P, Shetty A, Alland D, Rodrigues C. Xpert MTB/RIF: a New Pillar in Diagnosis of Extra-pulmonary Tuberculosis?, 2011; JOURNAL OF CLINICAL MICROBIOLOGY, July 2011, p. 2540–2545 Vol. 49, No. 7 0095-1137/11/$12.00 10.1128/JCM.02319-10 Copyright 2011, American Society for Microbiology. Available: http://jcm.asm.org/content/49/7/2540.short - DOI - PMC - PubMed
-
- World health Organization (2013). Global Tuberculosis report 2013, Available: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf?ua=1, Accessed 25 August 2014.
-
- Marais B, Hesseling A, Gie R, Schaaf H, Beyers N. The burden of childhood tuberculosis and the accuracy of community-based surveillance data. International Journal of Tuberculosis and Lung Disease, 2006; 10: 259–263. , Available: http://www.ncbi.nlm.nih.gov/pubmed/16562704. - PubMed
-
- Kumar A, Gupta D, Nagaraja S, Singh V, Sethi GR, Prasad J. Updated National Guidelines for Pediatric Tuberculosis in India, 2012. 2013; Indian Pediatr 50: 301–306. Available: http://www.indianpediatrics.net/mar2013/mar-301-306.htm - PubMed
-
- Revised National Tuberculosis Control Program. TB India 2015, RNTCP Annual Status Report, Reach the Unreached, 2015; Available: http://www.tbcindia.nic.in/pdfs/tb%20india%202014.pdf
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
