

Congenital syphilis: trends in mortality and morbidity in the United States, 1999 through 2013
- PMID: 26470826
- PMCID: PMC6463496
- DOI: 10.1016/j.ajog.2015.10.007
Congenital syphilis: trends in mortality and morbidity in the United States, 1999 through 2013
Abstract
Background: Congenital syphilis (CS) results when an infected pregnant mother transmits syphilis to her unborn child prior to or at delivery. The severity of infection can range from a delivery at term without signs of infection to stillbirth or death after delivery.
Objective: We sought to describe CS morbidity and mortality during 1999 through 2013.
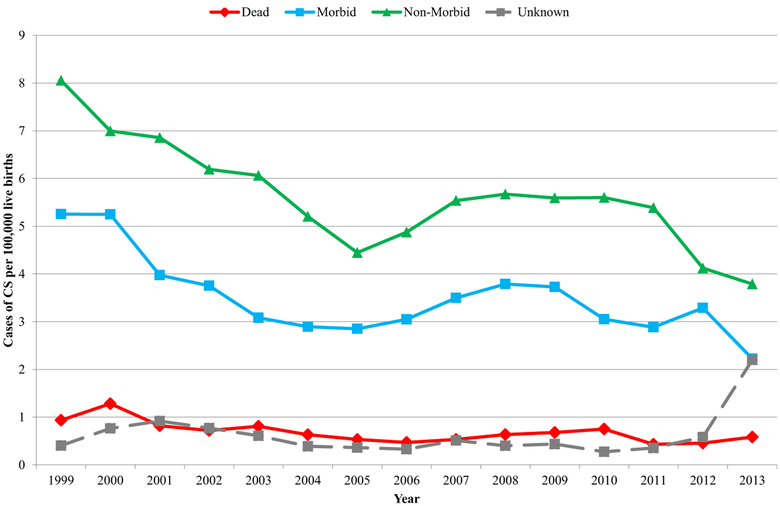
Study design: National CS case data reported to Centers for Disease Control and Prevention during 1999 through 2013 were analyzed. Cases were classified as dead (stillbirths and deaths up to 12 months after delivery), morbid (cases with strong [physical, radiographic, and/or nonserologic laboratory] evidence of CS), and nonmorbid (cases with a normal physical examination reported, without strong evidence of infection). Annual rates of these cases were calculated. Cases were compared using selected maternal and infant criteria.
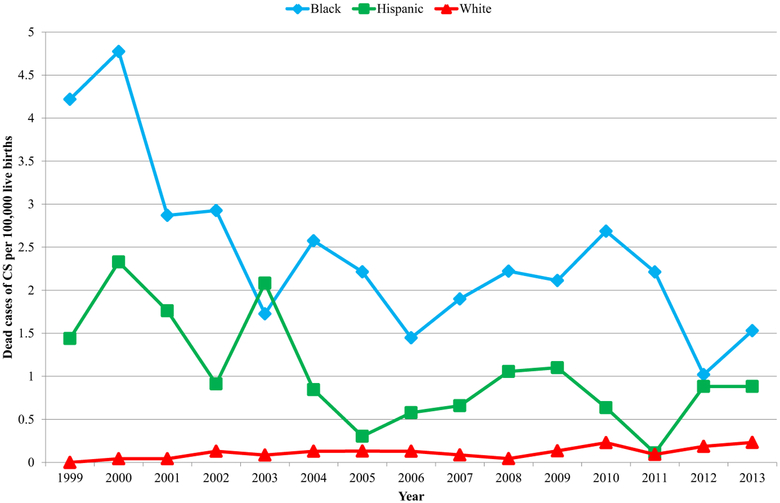
Results: During 1999 through 2013, 6383 cases of CS were reported: 6.5% dead, 33.6% morbid, 53.9% nonmorbid, and 5.9% unknown morbidity; 81.8% of dead cases were stillbirths. Rates of dead, morbid, and nonmorbid cases all decreased over this time period, but the overall proportions that were dead or morbid cases did not significantly change. The overall case fatality ratio during 1999 through 2013 was 6.5%. Among cases of CS, maternal race/ethnicity was not associated with increased morbidity or death, although most cases (83%) occurred among black or Hispanic mothers. No or inadequate treatment for maternal syphilis, <10 prenatal visits, and maternal nontreponemal titer ≥1:8 increased the likelihood of a dead case; risk of a dead case increased with maternal nontreponemal titer (χ(2) for trend P < .001). Infants with CS born alive at <28 weeks' gestation (relative risk, 107.4; P < .001) or born weighing <1500 g (relative risk, 43.9; P < .001) were at greatly increased risk of death.
Conclusion: CS remains an important preventable cause of perinatal morbidity and mortality, with comparable case fatality ratios during 1999 through 2013 (6.5%) and 1992 through 1998 (6.4%). Detection and treatment of syphilis early during pregnancy remain crucial to reducing CS morbidity and mortality.
Keywords: congenital syphilis; infant mortality; prenatal care; sexually transmitted disease surveillance; stillbirth.
Published by Elsevier Inc.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Ingraham NR Jr. The value of penicillin alone in the prevention and treatment of congenital syphilis. Acta Derm Venereol Suppl (Stockh) 1950;31(Suppl):60–87. - PubMed
-
- Alexander JM, Sheffield JS, Sanchez PJ, Mayfield J, Wendel GD Jr. Efficacy of treatment for syphilis in pregnancy. Obstet Gynecol 1999;93:5–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
