

CpG expedites regression of local and systemic tumors when combined with activatable nanodelivery
- PMID: 26471394
- PMCID: PMC4688109
- DOI: 10.1016/j.jconrel.2015.10.016
CpG expedites regression of local and systemic tumors when combined with activatable nanodelivery
Abstract
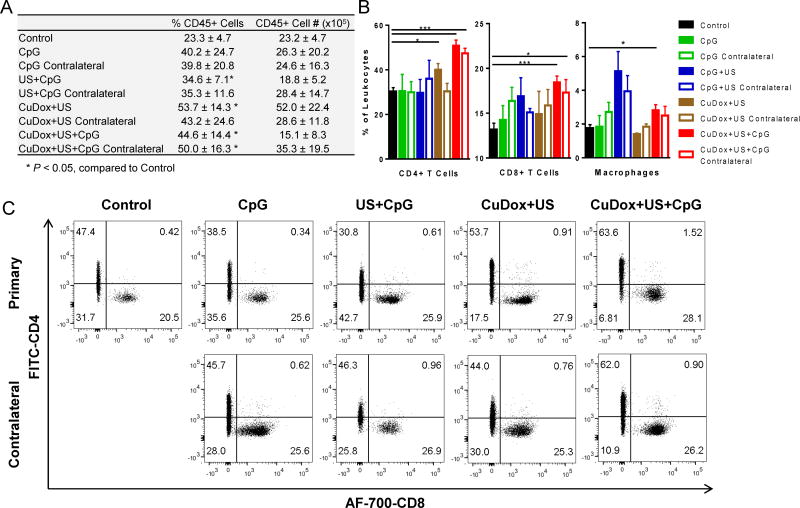
Ultrasonic activation of nanoparticles provides the opportunity to deliver a large fraction of the injected dose to insonified tumors and produce a complete local response. Here, we evaluate whether the local and systemic response to chemotherapy can be enhanced by combining such a therapy with locally-administered CpG as an immune adjuvant. In order to create stable, activatable particles, a complex between copper and doxorubicin (CuDox) was created within temperature-sensitive liposomes. Whereas insonation of the CuDox liposomes alone has been shown to produce a complete response in murine breast cancer after 8 treatments of 6 mg/kg delivered over 4 weeks, combining this treatment with CpG resolved local cancers within 3 treatments delivered over 7 days. Further, contralateral tumors regressed as a result of the combined treatment, and survival was extended in systemic disease. In both the treated and contralateral tumor site, the combined treatment increased leukocytes and CD4+ and CD8+ T-effector cells and reduced myeloid-derived suppressor cells (MDSCs). Taken together, the results suggest that this combinatorial treatment significantly enhances the systemic efficacy of locally-activated nanotherapy.
Keywords: CpG; Doxorubicin; Immunotherapy; Temperature-sensitive liposome; Ultrasound.
Copyright © 2015 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures










References
-
- Xu ZL, Zhu XQ, Lu P, Zhou Q, Zhang J, Wu F. Activation of tumor-infiltating antigen presenting cells by high intensity focused ultrasound ablation of human breast cancer. Ultrasound in Medicine and Biology. 2009;35:50–57. - PubMed
-
- Unga J, Hashida M. Ultrasound induced cancer immunotherapy. Advanced drug delivery reviews. 2014;72:144–153. - PubMed
-
- Weigel BJ, Rodeberg DA, Krieg AM, Blazar BR. CpG oligodeoxynucleotides potentiate the antitumor effects of chemotherapy or tumor resection in an orthotopic murine model of rhabdomyosarcoma. Clinical cancer research : an official journal of the American Association for Cancer Research. 2003;9:3105–3114. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
