

Fluid management guided by a continuous non-invasive arterial pressure device is associated with decreased postoperative morbidity after total knee and hip replacement
- PMID: 26471495
- PMCID: PMC4608292
- DOI: 10.1186/s12871-015-0131-8
Fluid management guided by a continuous non-invasive arterial pressure device is associated with decreased postoperative morbidity after total knee and hip replacement
Abstract
Background: The use of goal directed fluid protocols in intermediate risk patients undergoing hip or knee replacement was studied in few trials using invasive monitoring. For this reason we have implemented two different fluid management protocols, both based on a novel totally non-invasive arterial pressure monitoring device and compared them to the standard (no-protocol) treatment applied before the transition in our academic institution.
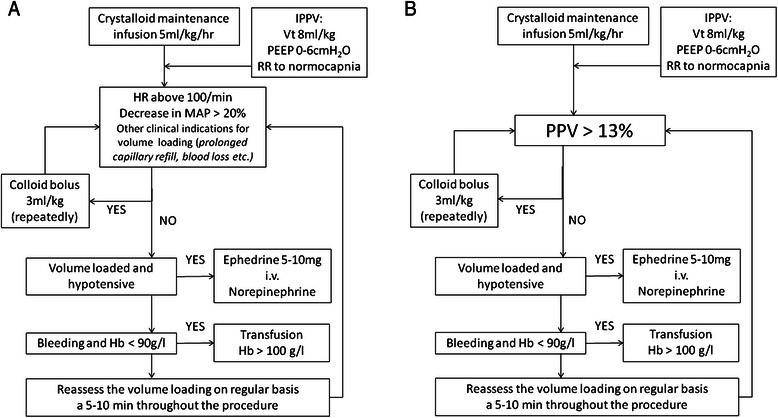
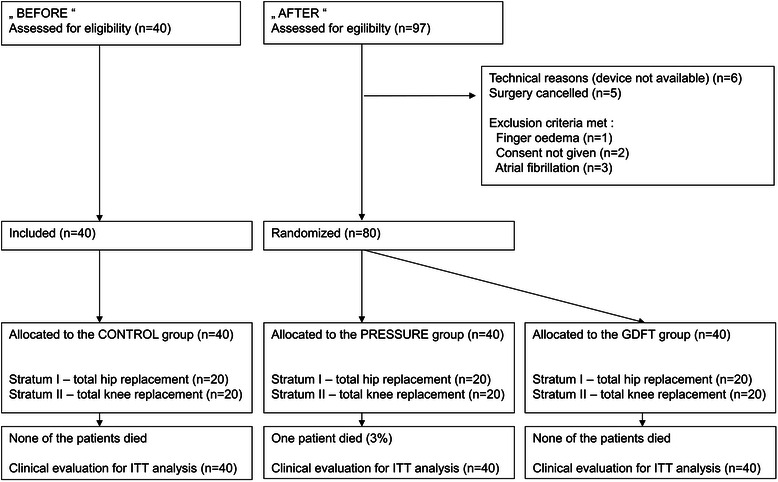
Methods: Three treatment groups were compared in this prospective study: the observational (CONTROL, N = 40) group before adoption of fluid protocols and two randomized groups after the transition to protocol fluid management with the use of the continuous non-invasive blood pressure monitoring (CNAP®) device. In the PRESSURE group (N = 40) standard variables were used for restrictive fluid therapy. Goal directed fluid therapy using pulse pressure variation was used in the GDFT arm (N = 40). The influence on the rate of postoperative complications, on the hospital length of stay and other parameters was assessed.
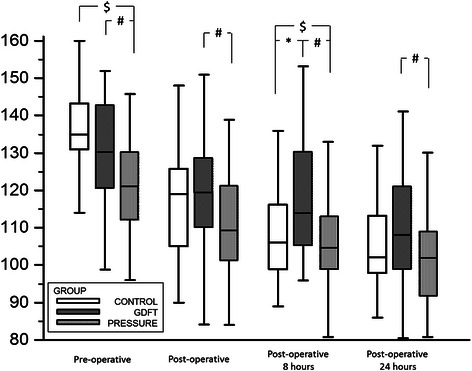
Results: Both protocols were associated with decreased fluid administration and maintained hemodynamic stability. Reduced rate of postoperative infection and organ complications (22 (55 %) vs. 33 (83 %) patients; p = 0.016; relative risk 0.67 (0.49-0.91)) was observed in the GDFT group compared to CONTROL. Lower number of patients receiving transfusion (4 (10 %) in GDFT vs. 17 (43 %) in CONTROL; p = 0.005) might contribute to this observation. No significant differences were observed in other end-points.
Conclusion: In our study, the use of the fluid protocol based on pulse pressure variation assessed using continuous non-invasive arterial pressure measurement seems to be associated with a reduction in postoperative complications and transfusion needs as compared to standard no-protocol treatment.
Trial registration: ACTRN12612001014842.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
