

Sarcopenia, sarcopenic obesity, and functional impairments in older adults: National Health and Nutrition Examination Surveys 1999-2004
- PMID: 26472145
- PMCID: PMC4825802
- DOI: 10.1016/j.nutres.2015.09.003
Sarcopenia, sarcopenic obesity, and functional impairments in older adults: National Health and Nutrition Examination Surveys 1999-2004
Abstract
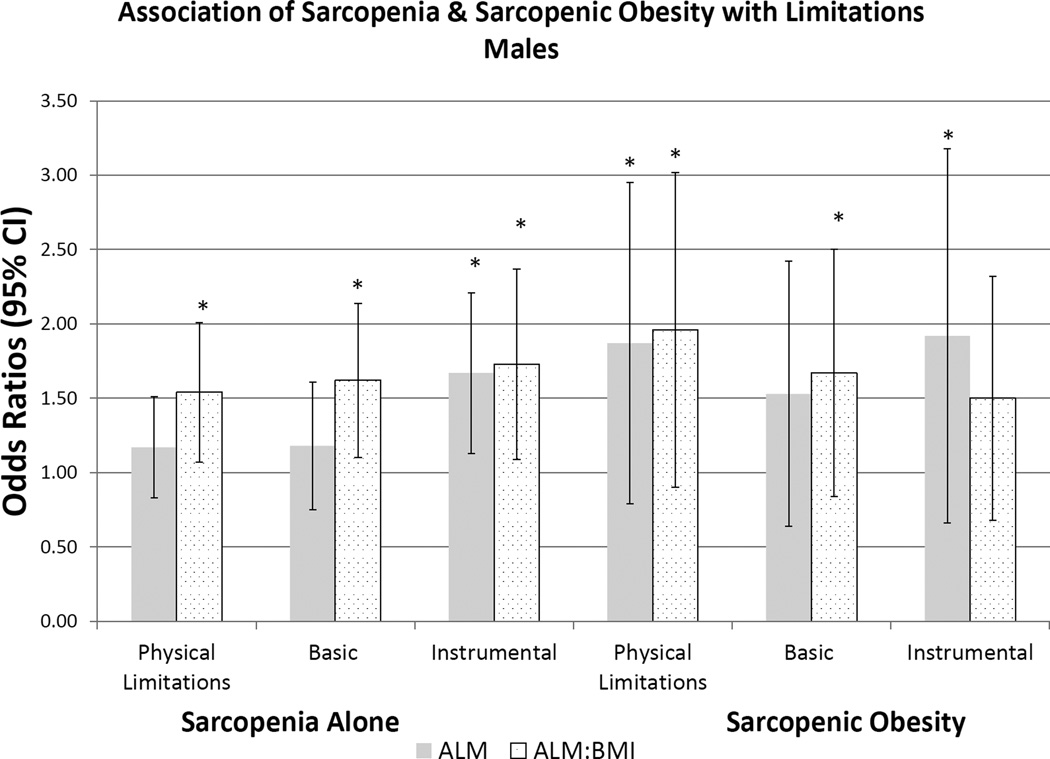
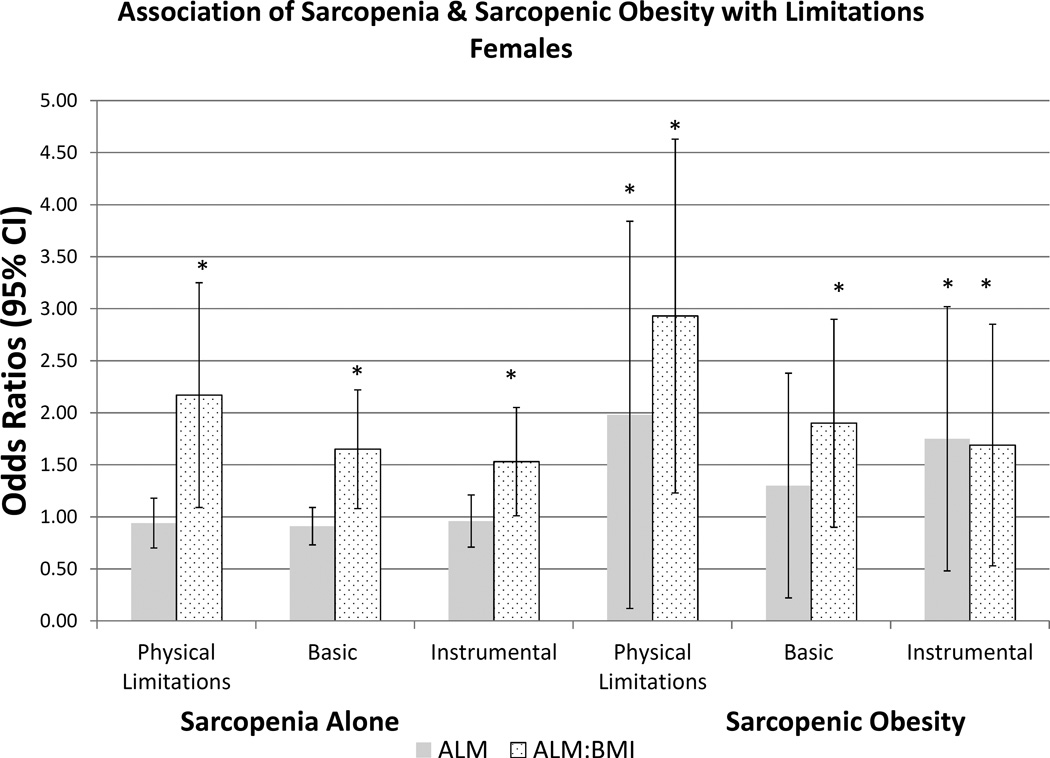
The Foundation for the National Institutes of Health Sarcopenia Project validated cutpoints for appendicular lean mass (ALM) to identify individuals with functional impairment. We hypothesized that the prevalence of sarcopenia and sarcopenic obesity would be similar based on the different Foundation for the National Institutes of Health criteria, increase with age, and be associated with risk of impairment limitations. We identified 4984 subjects at least 60 years of age from the National Health and Nutrition Examination Surveys 1999-2004. Sarcopenia was defined using ALM (men <19.75 kg, women <15.02 kg) and ALM adjusted for body mass index (BMI; men <0.789 kg/m2, women <0.512 kg/m2). Sarcopenic obesity is defined as subjects fulfilling the criteria for sarcopenia and obesity by body fat (men ≥25%, women ≥35%). Prevalence rates of both sarcopenia and sarcopenic obesity were evaluated with respect to sex, age category (60-69, 70-79, and >80 years) and race. We assessed the association of physical limitations, basic and instrumental activities of daily living and sarcopenia status. The mean age was 70.5 years in men and 71.6 years in women. Half (50.8%; n = 2531) were female, and mean BMI was 28 kg/m2 in both sexes. Appendicular lean mass was higher in men than in women (24.1 vs. 16.3; P < .001), but fat mass was lower (30.9 vs. 42.0; P < .001). In men, sarcopenia prevalence was 16.0% and 27.8% using the ALM and ALM/BMI criteria. In women, prevalence was 40.5% and 19.3% using the ALM and ALM/BMI criteria. Sarcopenia was associated with a 1.10 (0.86-1.41) and 0.93 (0.74-1.16), and 1.46 (1.10-1.94), and 2.13 (1.41-3.20) risk of physical limitations using the ALM and ALM/BMI definitions in men and women, respectively. Prevalence of sarcopenia and sarcopenic obesity varies greatly, and a uniform definition is needed to identify and characterize these high-risk populations.
Keywords: Body fat; Epidemiology; Function; Obesity; Sarcopenia.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
