

Contributions of Subtypes of Non-Hodgkin Lymphoma to Mortality Trends
- PMID: 26472423
- PMCID: PMC4713325
- DOI: 10.1158/1055-9965.EPI-15-0921
Contributions of Subtypes of Non-Hodgkin Lymphoma to Mortality Trends
Abstract
Background: Non-Hodgkin lymphoma (NHL) comprises distinct tumor subtypes. Although mortality from NHL overall has changed dramatically in the United States over time, little is known about trends for subtypes, because death certificates do not record this information.
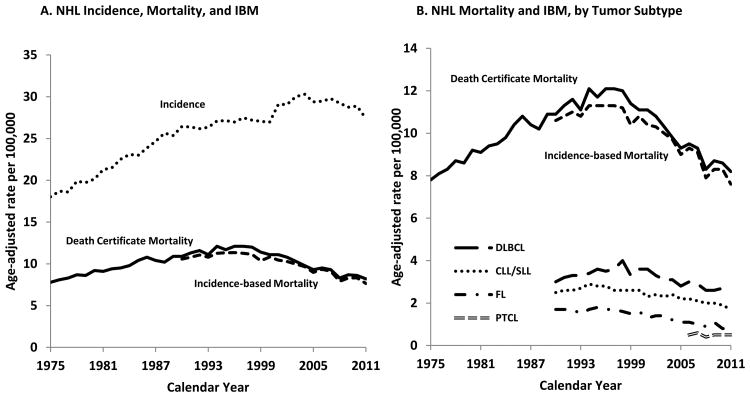
Methods: Using data from U.S. Surveillance, Epidemiology, and End Results (SEER) areas, we assessed NHL mortality rates and mapped NHL deaths to incident NHL cases in SEER cancer registries. This allowed us to evaluate population-level mortality trends attributed to specific NHL subtypes (incidence-based mortality; IBM). We also describe NHL incidence and survival after NHL diagnosis by calendar year. We used Joinpoint to identify years when IBM and incidence rate trends changed slope.
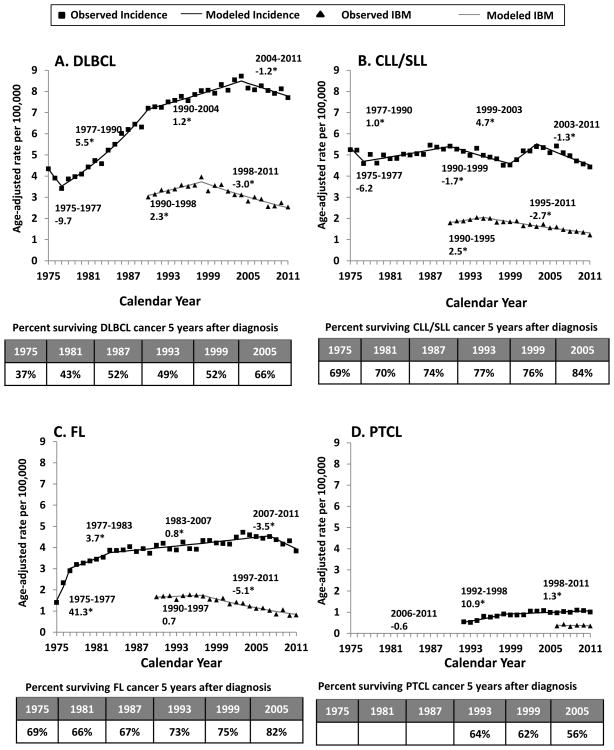
Results: Overall NHL mortality rates increased during 1975-1997, peaking at 10.9 per 100,000 person-years, then decreased subsequently in 1997-2011. Overall IBM rates mirror this trend during 1990-2011. For B-cell NHL subtypes, IBM rates decreased beginning in the mid-1990s, with yearly declines of -3.0% for diffuse large B-cell lymphoma (DLBCL), -2.7% for chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), and -5.3% for follicular lymphoma. Incidence rates for these subtypes did not decrease until after 2003. Corresponding 5-year cancer-specific survival increased dramatically over time for DLBCL (from 37%-66%), CLL/SLL (69%-84%), and follicular lymphoma (69%-82%). IBM for peripheral T-cell lymphoma was flat during 2006-2011, although incidence increased.
Conclusions: Mortality due to three common B-cell NHL subtypes has fallen over time in the United States.
Impact: This decline reflects better survival after NHL diagnosis, likely from improved therapies, because the decline in NHL incidence occurred later.
©2015 American Association for Cancer Research.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Jaffe ESHN, Stein H, Vardiman JW, editors. World Health Organization Classification of Tumours Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2001.
-
- Howlader N, Noone Anne-Michelle, Krapcho M. SEER Cancer Statistics Review (CSR) 1975-2011. available from: http://seer.cancer.gov/csr/1975_2011/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
