

The offering of family presence during resuscitation: a systematic review and meta-analysis
- PMID: 26473034
- PMCID: PMC4607174
- DOI: 10.1186/s40560-015-0107-2
The offering of family presence during resuscitation: a systematic review and meta-analysis
Abstract
Background: Family members may wish to be present during resuscitation of loved ones, despite concerns that they may interfere with the resuscitation or experience psychological harm.
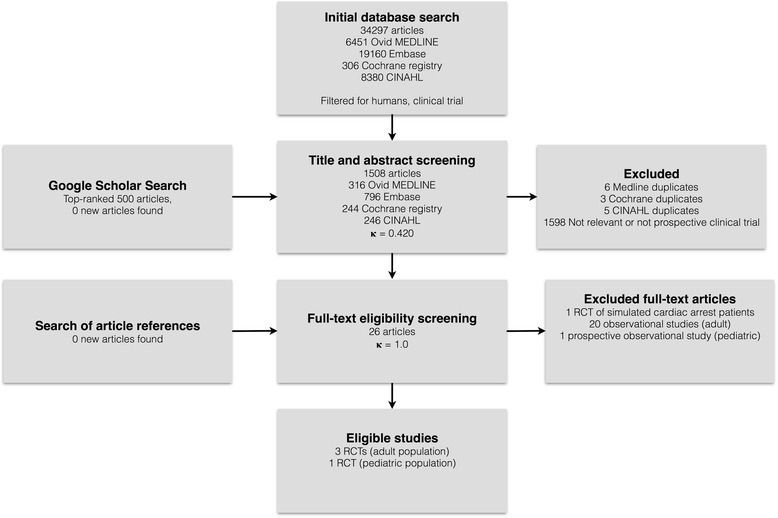
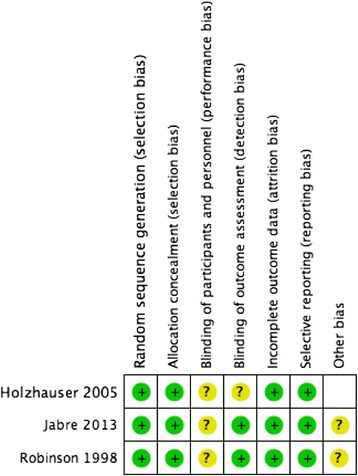
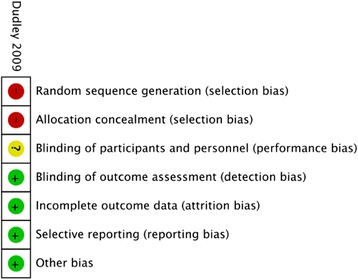
Methods: We conducted a systematic review to determine whether offering family presence during resuscitation (FPDR) affected patient mortality, resuscitation quality, or family member psychological outcomes. We searched multiple databases up to January 2014 for studies comparing FPDR to usual care. Two reviewers independently assessed eligibility, risk of bias, and extracted data. Data from randomized controlled trial (RCTs) at low or uncertain risk of bias were eligible for pooling. Quality of evidence was assessed using GRADE.
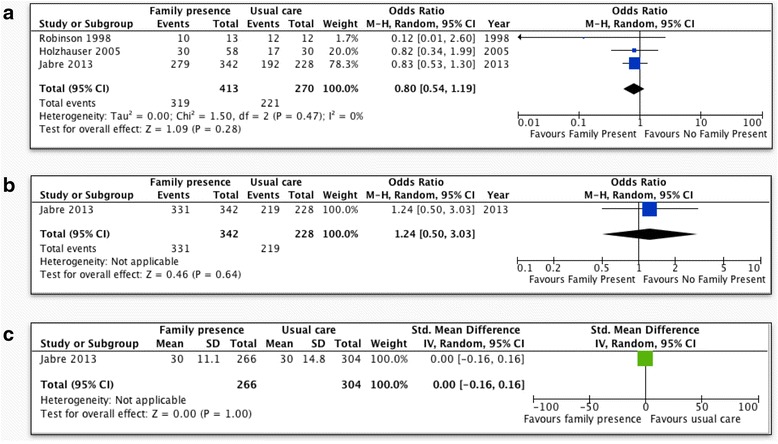
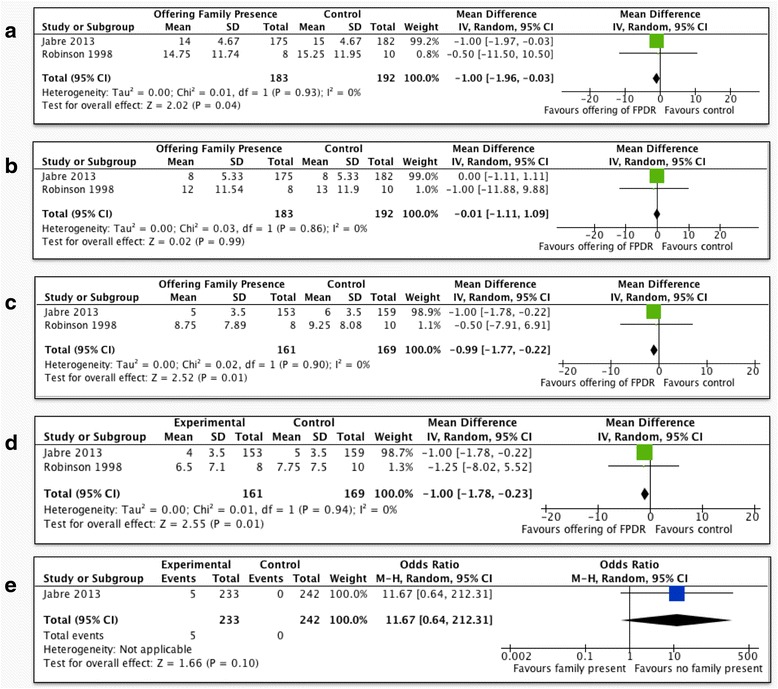
Results: Three RCTs evaluated the offering of FPDR in adults, finding no differences in resuscitation duration, prehospital/emergency room mortality (odds ratio [OR] 0.80, 95 % confidence interval [CI] 0.54-1.19), or 28-day mortality (OR 1.24, 95 % CI [0.50-3.03]). Hospital Anxiety and Depression Scale scores for anxiety (mean difference [MD] -0.99, 95 % CI [-1.77, -0.22]) and depression (MD -1.00, 95 % CI [-1.78, -0.23]), along with Impact of Events Scale intrusion score (MD -1.00, 95 % CI [-1.96, -0.03]), were better in family members offered FPDR. One RCT evaluated FPDR in pediatric patients, finding no mortality differences at 28 days (OR 0.30; 95 % CI [0.11-0.79]), but did not report psychological outcomes in family members.
Conclusions: Moderate-quality evidence suggests the offering of FPDR does not affect adult resuscitation outcomes and may improve family member psychological outcomes. Low-quality evidence suggests FPDR does not affect pediatric resuscitation outcomes. The generalizability of these findings outside the prehospital and emergency room setting is limited due to the absence of trials in other health care settings.
Keywords: Family; Family presence; Family-centered care; Resuscitation.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
