

Liver Fat Content Is Associated with Elevated Serum Uric Acid in the Chinese Middle-Aged and Elderly Populations: Shanghai Changfeng Study
- PMID: 26473493
- PMCID: PMC4608581
- DOI: 10.1371/journal.pone.0140379
Liver Fat Content Is Associated with Elevated Serum Uric Acid in the Chinese Middle-Aged and Elderly Populations: Shanghai Changfeng Study
Abstract
Background and aims: Although many studies have indicated a relationship between nonalcoholic fatty liver disease (NAFLD) and hyperuricemia, a few studies specifically examining the effects of the severity of liver fat content (LFC) on serum uric acid (SUA) and the presence of hyperuricemia because of the limitation of the examination methods for NAFLD. In this study, we investigate the relationship between the NAFLD and SUA levels in the Chinese population using standardized quantitative ultrasound.
Methods: A community-based study was conducted from May 2010 to December 2012. A total of 4,305 people aged 45 years and above without excessive drinking were enrolled. A standard interview and anthropometric and laboratory blood parameters were collected for each person. The standardized ultrasound hepatic/renal ratio and hepatic attenuation rate was used to quantify LFC.
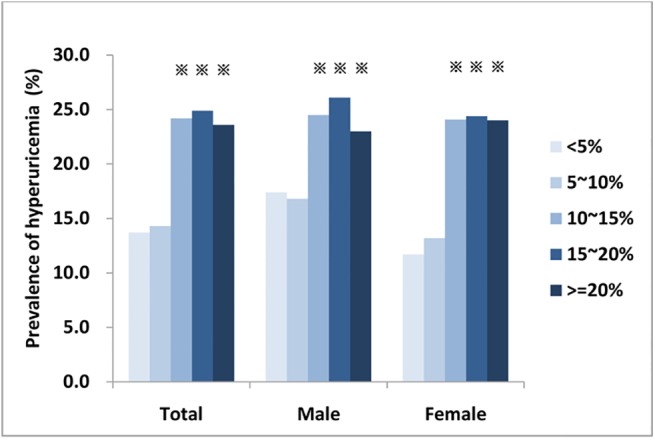
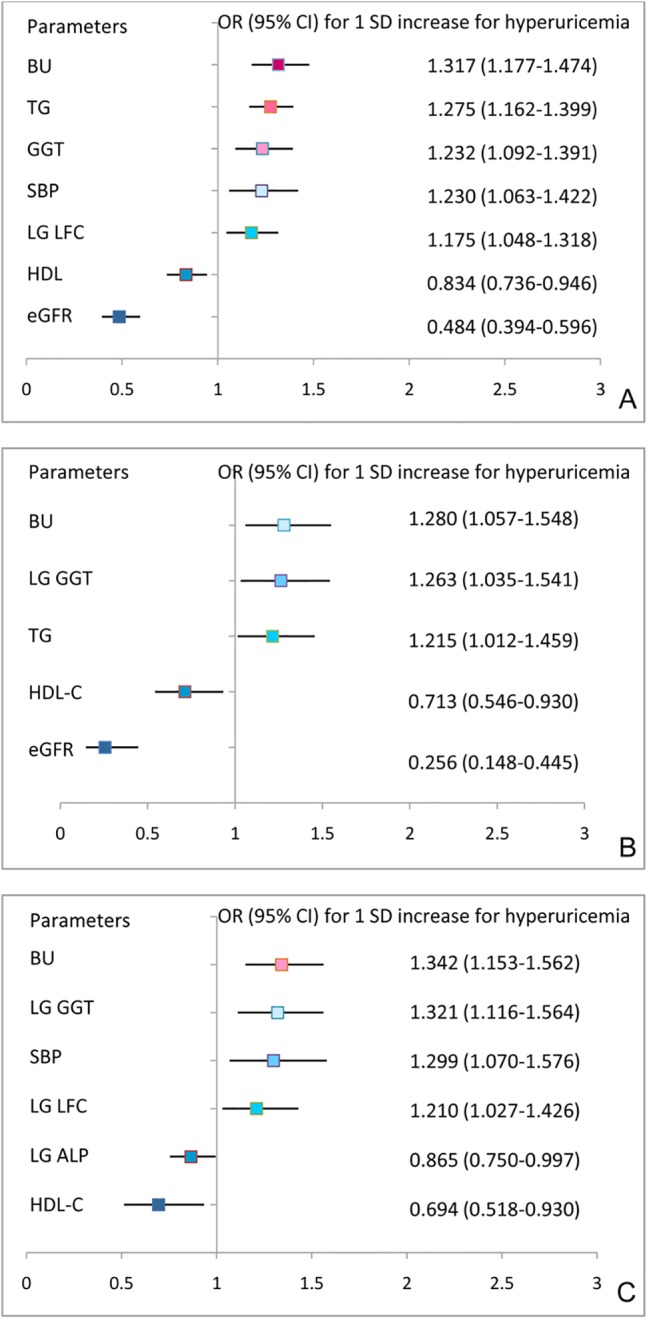
Results: The prevalence of NAFLD and hyperuricemia was 33.1% and 17.1%, respectively. A total of 23.5% of the NAFLD subjects had hyperuricemia, and their SUA was higher than that of non-NAFLD subjects (327.2 ± 76.8 vs 301.9 ± 77.4 μmol/L, P < 0.001). The LFC was positively correlated with SUA (r = 0.130, P < 0.001) and an independent factor for SUA (standardized β = 0.054, P < 0.001). The OR for the presence of hypreuricemia was 1.175 (95% CI 1.048-1.318; P < 0.001) with a 1 SD increase in the log LFC. LFC greater than 10% was related to elevated SUA and an increased presence of hyperuricemia.
Conclusions: LFC accumulation was associated with an increase in the prevalence of hyperuricemia and elevated SUA in our community-based population. LFC greater than 10% is related to the risk for hyperuricemia.
Conflict of interest statement
Figures
Similar articles
-
Serum uric acid and non-alcoholic fatty liver disease in non-obesity Chinese adults.Lipids Health Dis. 2017 Oct 16;16(1):202. doi: 10.1186/s12944-017-0531-5. Lipids Health Dis. 2017. PMID: 29037239 Free PMC article.
-
[Relationship between normal serum uric acid levels and nonalcoholic fatty liver disease in postmenopausal women].Zhonghua Gan Zang Bing Za Zhi. 2014 Jan;22(1):53-7. doi: 10.3760/cma.j.issn.1007-3418.2014.01.012. Zhonghua Gan Zang Bing Za Zhi. 2014. PMID: 24721245 Chinese.
-
Association between serum uric acid and nonalcoholic fatty liver disease in the US population.J Formos Med Assoc. 2015 Apr;114(4):314-20. doi: 10.1016/j.jfma.2012.11.014. Epub 2013 Jan 11. J Formos Med Assoc. 2015. PMID: 25839764 Free PMC article.
-
Can Serum Uric Acid Lowering Therapy Contribute to the Prevention or Treatment of Nonalcoholic Fatty Liver Disease?Curr Vasc Pharmacol. 2018;16(3):269-275. doi: 10.2174/1570161115666170621082237. Curr Vasc Pharmacol. 2018. PMID: 28676018 Review.
-
Serum uric acid: a new therapeutic target for nonalcoholic fatty liver disease.Expert Opin Ther Targets. 2016;20(3):375-87. doi: 10.1517/14728222.2016.1096930. Epub 2015 Sep 30. Expert Opin Ther Targets. 2016. PMID: 26419119 Review.
Cited by
-
Metformin attenuates triglyceride accumulation in HepG2 cells through decreasing stearyl-coenzyme A desaturase 1 expression.Lipids Health Dis. 2018 May 14;17(1):114. doi: 10.1186/s12944-018-0762-0. Lipids Health Dis. 2018. PMID: 29759071 Free PMC article.
-
Nonlinear Association Between the Liver Fat Content and the Risk of Hyperuricemia in Prediabetic Individuals: Evidence from Cross-Sectional Health Screening Data in China.Diabetes Metab Syndr Obes. 2025 Feb 12;18:423-434. doi: 10.2147/DMSO.S506893. eCollection 2025. Diabetes Metab Syndr Obes. 2025. PMID: 39963192 Free PMC article.
-
Value of Visceral Fat Area and Resting Energy Expenditure in Assessment of Metabolic Characteristics in Obese and Lean Nonalcoholic Fatty Liver Disease.Turk J Gastroenterol. 2021 Feb;32(2):116-122. doi: 10.5152/tjg.2021.20908. Turk J Gastroenterol. 2021. PMID: 33960934 Free PMC article.
-
Association between serum uric acid and nonalcoholic fatty liver disease in community patients with type 2 diabetes mellitus.PeerJ. 2019 Aug 26;7:e7563. doi: 10.7717/peerj.7563. eCollection 2019. PeerJ. 2019. PMID: 31523513 Free PMC article.
-
The correlation between controlled attenuation parameter and metabolic syndrome and its components in middle-aged and elderly nonalcoholic fatty liver disease patients.Medicine (Baltimore). 2018 Oct;97(43):e12931. doi: 10.1097/MD.0000000000012931. Medicine (Baltimore). 2018. PMID: 30412101 Free PMC article.
References
-
- Katsiki N, Papanas N, Fonseca VA, Maltezos E, Mikhailidis DP (2013) Uric acid and diabetes: Is there a link? Curr Pharm Des 19: 4930–4937. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
