

Comparison of Two Sepsis Recognition Methods in a Pediatric Emergency Department
- PMID: 26474032
- PMCID: PMC4639443
- DOI: 10.1111/acem.12814
Comparison of Two Sepsis Recognition Methods in a Pediatric Emergency Department
Abstract
Objectives: The objective was to compare the effectiveness of physician judgment and an electronic algorithmic alert to identify pediatric patients with severe sepsis/septic shock in a pediatric emergency department (ED).
Methods: This was an observational cohort study of patients older than 56 days with fever or hypothermia. All patients were evaluated for potential sepsis in real time by the ED clinical team. An electronic algorithmic alert was retrospectively applied to identify patients with potential sepsis independent of physician judgment. The primary outcome was the proportion of patients correctly identified with severe sepsis/septic shock defined by consensus criteria. Test characteristics were determined and receiver operating characteristic (ROC) curves were compared.
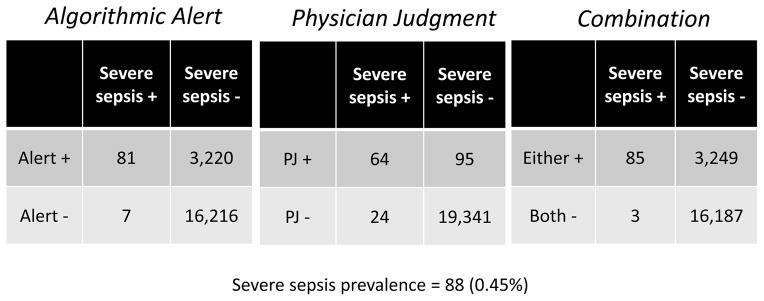
Results: Of 19,524 eligible patient visits, 88 patients developed consensus-confirmed severe sepsis or septic shock. Physician judgment identified 159 and the algorithmic alert identified 3,301 patients with potential sepsis. Physician judgment had sensitivity of 72.7% (95% confidence interval [CI] = 72.1% to 73.4%) and specificity of 99.5% (95% CI = 99.4% to 99.6%); the algorithmic alert had sensitivity of 92.1% (95% CI = 91.7% to 92.4%) and specificity of 83.4% (95% CI = 82.9% to 83.9%) for severe sepsis/septic shock. There was no significant difference in the area under the ROC curve for physician judgment (0.86, 95% CI = 0.81 to 0.91) or the algorithm (0.88, 95% CI = 0.85 to 0.91; p = 0.54). A combination method using either positive physician judgment or an algorithmic alert improved sensitivity to 96.6% and specificity to 83.3%. A sequential approach, in which positive identification by the algorithmic alert was then confirmed by physician judgment, achieved 68.2% sensitivity and 99.6% specificity. Positive and negative predictive values for physician judgment versus algorithmic alert were 40.3% versus 2.5% and 99.88% versus 99.96%, respectively.
Conclusions: The electronic algorithmic alert was more sensitive but less specific than physician judgment for recognition of pediatric severe sepsis and septic shock. These findings can help to guide institutions in selecting pediatric sepsis recognition methods based on institutional needs and priorities.
© 2015 by the Society for Academic Emergency Medicine.
Figures
Similar articles
-
Diagnostic accuracy of a screening electronic alert tool for severe sepsis and septic shock in the emergency department.BMC Med Inform Decis Mak. 2014 Dec 5;14:105. doi: 10.1186/s12911-014-0105-7. BMC Med Inform Decis Mak. 2014. PMID: 25476738 Free PMC article.
-
Validation of the Pediatric Sequential Organ Failure Assessment Score and Evaluation of Third International Consensus Definitions for Sepsis and Septic Shock Definitions in the Pediatric Emergency Department.JAMA Pediatr. 2022 Jul 1;176(7):672-678. doi: 10.1001/jamapediatrics.2022.1301. JAMA Pediatr. 2022. PMID: 35575803 Free PMC article.
-
Improving Recognition of Pediatric Severe Sepsis in the Emergency Department: Contributions of a Vital Sign-Based Electronic Alert and Bedside Clinician Identification.Ann Emerg Med. 2017 Dec;70(6):759-768.e2. doi: 10.1016/j.annemergmed.2017.03.019. Epub 2017 Jun 2. Ann Emerg Med. 2017. PMID: 28583403 Free PMC article.
-
Racial Differences in Sepsis Recognition in the Emergency Department.Pediatrics. 2019 Oct;144(4):e20190348. doi: 10.1542/peds.2019-0348. Epub 2019 Sep 13. Pediatrics. 2019. PMID: 31519793
-
Development of a New Screening Tool for Pediatric Septic Shock.Ann Emerg Med. 2024 Dec;84(6):642-650. doi: 10.1016/j.annemergmed.2024.06.026. Epub 2024 Aug 1. Ann Emerg Med. 2024. PMID: 39093249
Cited by
-
2016 Update for the Rogers' Textbook of Pediatric Intensive Care: Recognition and Initial Management of Shock.Pediatr Crit Care Med. 2016 Nov;17(11):1073-1079. doi: 10.1097/PCC.0000000000000942. Pediatr Crit Care Med. 2016. PMID: 27749512 Free PMC article. Review.
-
Multidisciplinary Kaizen Event to Improve Adherence to a Sepsis Clinical Care Guideline.Pediatr Qual Saf. 2021 Jun 23;6(4):e435. doi: 10.1097/pq9.0000000000000435. eCollection 2021 Jul-Aug. Pediatr Qual Saf. 2021. PMID: 34235357 Free PMC article.
-
[Paediatric Life Support].Notf Rett Med. 2021;24(4):650-719. doi: 10.1007/s10049-021-00887-9. Epub 2021 Jun 2. Notf Rett Med. 2021. PMID: 34093080 Free PMC article. Review. German.
-
Paediatric patient stratification in the emergency department.Lancet Child Adolesc Health. 2020 Aug;4(8):557-558. doi: 10.1016/S2352-4642(20)30208-X. Epub 2020 Jul 22. Lancet Child Adolesc Health. 2020. PMID: 32710836 Free PMC article. No abstract available.
-
Early Experience with a Novel Strategy for Assessment of Sepsis Risk: The Shock Huddle.Pediatr Qual Saf. 2019 Jul 22;4(4):e197. doi: 10.1097/pq9.0000000000000197. eCollection 2019 Jul-Aug. Pediatr Qual Saf. 2019. PMID: 31572898 Free PMC article.
References
-
- Lilly CM. The ProCESS trial--a new era of sepsis management. N Engl J Med. 2014;370(18):1750–1. - PubMed
-
- Launay E, Gras-Le Guen C, Martinot A, et al. Suboptimal care in the initial management of children who died from severe bacterial infection: a population-based confidential inquiry. Pediatr Crit Care Med. 2010;11(4):469–74. - PubMed
-
- de Oliveira CF, de Oliveira DS, Gottschald AF, et al. ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous oxygen saturation. Intensive Care Med. 2008;34(6):1065–75. - PubMed
-
- Cruz AT, Perry AM, Williams EA, Graf JM, Wuestner ER, Patel B. Implementation of goal-directed therapy for children with suspected sepsis in the emergency department. Pediatrics. 2011;127(3):e758–66. - PubMed
-
- Larsen GY, Mecham N, Greenberg R. An emergency department septic shock protocol and care guideline for children initiated at triage. Pediatrics. 2011;127(6):e1585–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
