

Timing of Intubation and Clinical Outcomes in Adults With Acute Respiratory Distress Syndrome
- PMID: 26474112
- PMCID: PMC4774861
- DOI: 10.1097/CCM.0000000000001359
Timing of Intubation and Clinical Outcomes in Adults With Acute Respiratory Distress Syndrome
Abstract
Objective: The prevalence, clinical characteristics, and outcomes of critically ill, nonintubated patients with evidence of the acute respiratory distress syndrome remain inadequately characterized.
Design: Secondary analysis of a prospective observational cohort study.
Setting: Vanderbilt University Medical Center.
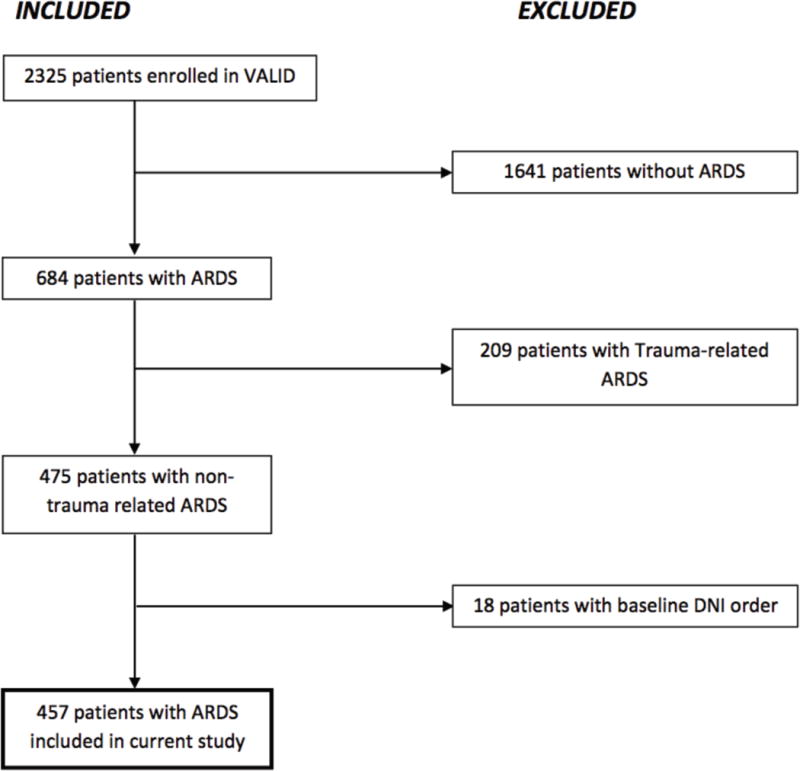
Patients: Among adult patients enrolled in a large, multi-ICU prospective cohort study between the years of 2006 and 2011, we studied intubated and nonintubated patients with acute respiratory distress syndrome as defined by acute hypoxemia (PaO2/FIO2 ≤ 300 or SpO2/FIO2 ≤ 315) and bilateral radiographic opacities not explained by cardiac failure. We excluded patients not committed to full respiratory support.
Interventions: None.
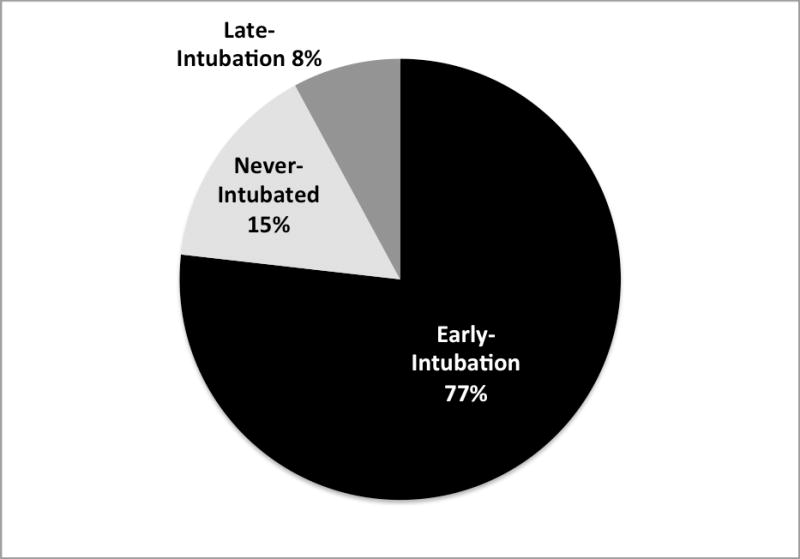
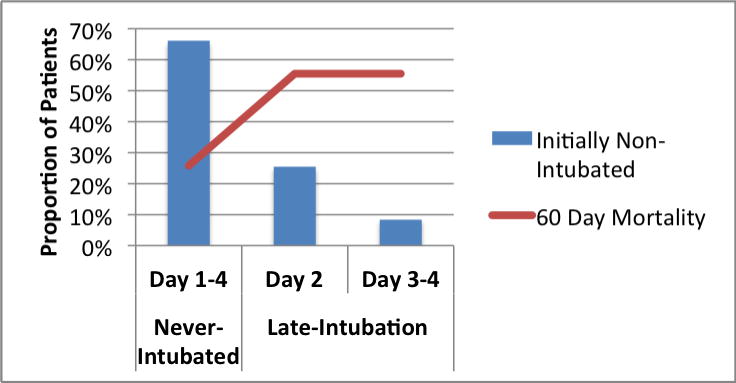
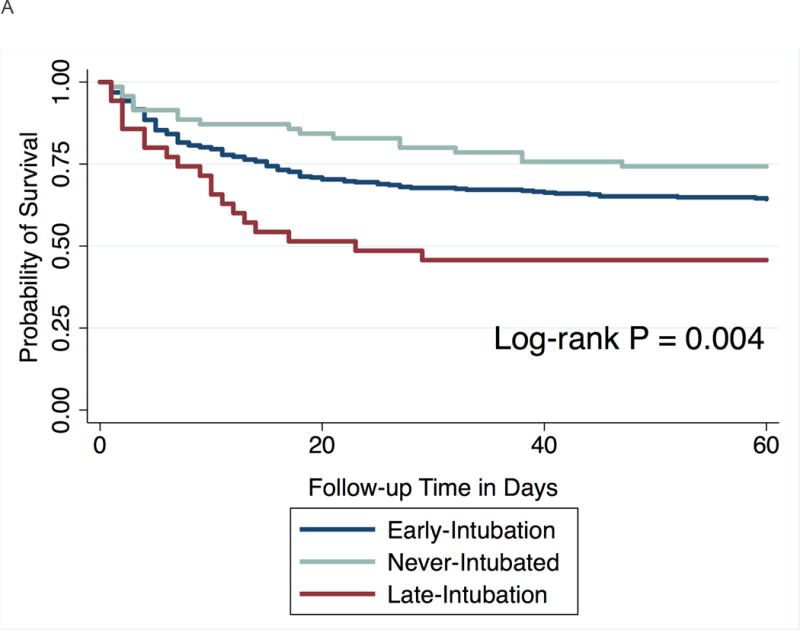
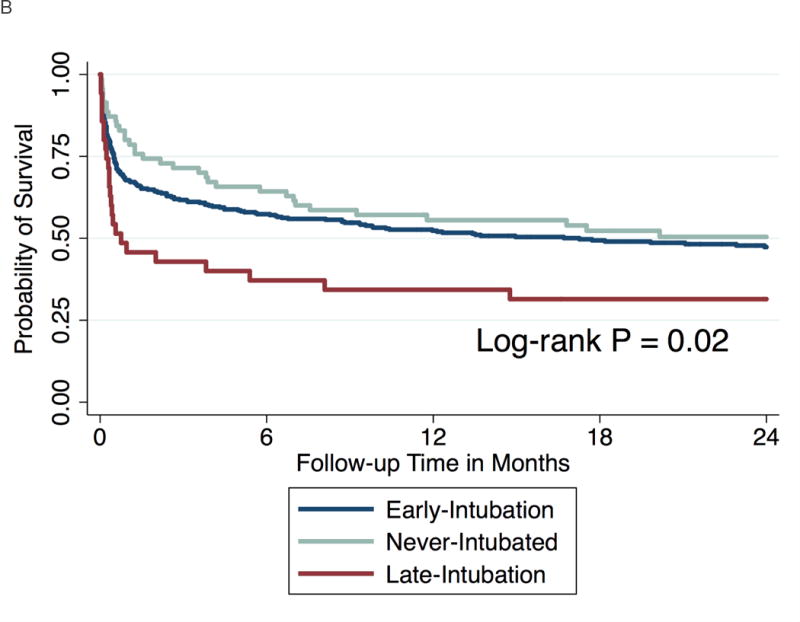
Measurements and main results: Of 457 patients with acute respiratory distress syndrome, 106 (23%) were not intubated at the time of meeting all other acute respiratory distress syndrome criteria. Nonintubated patients had lower morbidity and severity of illness than intubated patients; however, mortality at 60 days was the same (36%) in both groups (p = 0.91). Of the 106 nonintubated patients, 36 (34%) required intubation within the subsequent 3 days of follow-up; this late-intubation subgroup had significantly higher 60-day mortality (56%) when compared with the both early intubation group (36%, P<0.03) and patients never requiring intubation (26%; p = 0.002). Increased mortality in the late intubation group persisted at 2-year follow-up. Adjustment for baseline clinical and demographic differences did not change the results.
Conclusions: A substantial proportion of critically ill adults with acute respiratory distress syndrome were not intubated in their initial days of intensive care, and many were never intubated. Late intubation was associated with increased mortality. Criteria defining the acute respiratory distress syndrome prior to need for positive pressure ventilation are required so that these patients can be enrolled in clinical studies and to facilitate early recognition and treatment of acute respiratory distress syndrome.
Conflict of interest statement
No author (KNK, LBW, CW, DRJ, HZ, MAM, CSC) reports a conflict of interest.
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Nonintubated Patients With Acute Respiratory Distress Syndrome: A Watchful Evaluation.Crit Care Med. 2016 Jan;44(1):246-7. doi: 10.1097/CCM.0000000000001438. Crit Care Med. 2016. PMID: 26672935 No abstract available.
-
High-Flow Oxygen as Noninvasive Ventilation May Complicate Timely Intubation in Patients With Acute Respiratory Distress Syndrome.Crit Care Med. 2016 Aug;44(8):e768-9. doi: 10.1097/CCM.0000000000001782. Crit Care Med. 2016. PMID: 27428147 No abstract available.
-
The authors reply.Crit Care Med. 2016 Aug;44(8):e769-70. doi: 10.1097/CCM.0000000000001910. Crit Care Med. 2016. PMID: 27428148 Free PMC article. No abstract available.
-
Exploring Causative Pathology Is Essential for Validating Harmful Effects of Late Intubation.Crit Care Med. 2016 Aug;44(8):e770-1. doi: 10.1097/CCM.0000000000001787. Crit Care Med. 2016. PMID: 27428149 No abstract available.
-
The authors reply.Crit Care Med. 2016 Aug;44(8):e771. doi: 10.1097/CCM.0000000000001909. Crit Care Med. 2016. PMID: 27428150 Free PMC article. No abstract available.
References
-
- Ashbaugh DG, Bigelow DB, Petty TL, et al. Acute respiratory distress in adults. Lancet. 1967;2(7511):319–323. - PubMed
-
- Bell RC, Coalson JJ, Smith JD, et al. Multiple organ system failure and infection in adult respiratory distress syndrome. Ann Intern Med. 1983;99(3):293–298. - PubMed
-
- Fowler AA, Hamman RF, Good JT, et al. Adult respiratory distress syndrome: risk with common predispositions. Ann Intern Med. 1983;98(5 Pt 1):593–597. - PubMed
-
- Pepe PE, Potkin RT, Reus DH, et al. Clinical predictors of the adult respiratory distress syndrome. Am J Surg. 1982;144(1):124–130. - PubMed
-
- Sloane PJ, Gee MH, Gottlieb JE, et al. A multicenter registry of patients with acute respiratory distress syndrome. Physiology and outcome. Am Rev Respir Dis. 1992;146(2):419–426. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
