

Neighbourhood socio-economic status and all-cause mortality in adults with atrial fibrillation: A cohort study of patients treated in primary care in Sweden
- PMID: 26474468
- PMCID: PMC4679195
- DOI: 10.1016/j.ijcard.2015.09.027
Neighbourhood socio-economic status and all-cause mortality in adults with atrial fibrillation: A cohort study of patients treated in primary care in Sweden
Abstract
Objective: Our aim was to study the potential impact of neighbourhood socio-economic status (SES) on all-cause mortality in patients with atrial fibrillation (AF) treated in primary care.
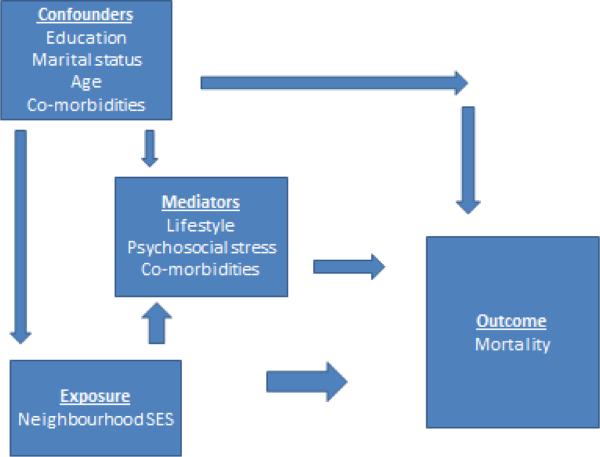
Methods: Study population included adults (n=12,283) of 45 years and older diagnosed with AF in 75 primary care centres in Sweden. Association between neighbourhood SES and all-cause mortality was explored using Cox regression analysis, with hazard ratios (HRs) and 95% confidence intervals (95% CIs), and by Laplace regression where years to death (95% CI) of the first 10% of the participants were used as an outcome. All models were conducted in both men and women and adjusted for age, educational level, marital status, change of neighbourhood status, cardiovascular co-morbidities, anticoagulant treatment and statin treatment. High- and low-neighbourhood SES were compared with middle SES as reference group.
Results: After adjustments for potential confounders, higher relative risk of all-cause mortality (HR 1.49, 95% CI 1.13-1.96) was observed in men living in low SES neighbourhoods compared to those from middle SES neighbourhoods. The results were confirmed using Laplace regression; the time until the first 10% of the men in low SES neighbourhoods died was 1.45 (95% CI 0.48-2.42) years shorter than for the men in middle SES neighbourhoods.
Conclusions: Increased rates of heart disease and subsequent mortality among adults in deprived neighbourhoods raise important clinical and public health concerns. These findings could serve as an aid to policy-makers when allocating resources in primary health care settings as well as to clinicians who encounter patients in deprived neighbourhoods.
Keywords: Antithrombotic drugs; Atrial fibrillation; Co-morbidity; Follow-up; Gender; Mortality; Neighbourhood.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr., et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–2104. - PubMed
-
- Forslund T, Wettermark B, Wandell P, von Euler M, Hasselstrom J, Hjemdahl P. Risk scoring and thromboprophylactic treatment of patients with atrial fibrillation with and without access to primary healthcare data: experience from the Stockholm health care system. Int J Cardiol. 2013;170:208–214. - PubMed
-
- Bajpai A, Savelieva I, Camm AJ. Treatment of atrial fibrillation. Br Med Bull. 2008;88:75–94. - PubMed
-
- Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998;82:2N–9N. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
