

Echocardiographic Algorithm for Post-Myocardial Infarction LV Thrombus: A Gatekeeper for Thrombus Evaluation by Delayed Enhancement CMR
- PMID: 26476503
- PMCID: PMC5104336
- DOI: 10.1016/j.jcmg.2015.06.017
Echocardiographic Algorithm for Post-Myocardial Infarction LV Thrombus: A Gatekeeper for Thrombus Evaluation by Delayed Enhancement CMR
Abstract
Objectives: The goal of this study was to determine the prevalence of post-myocardial infarction (MI) left ventricular (LV) thrombus in the current era and to develop an effective algorithm (predicated on echocardiography [echo]) to discern patients warranting further testing for thrombus via delayed enhancement (DE) cardiac magnetic resonance (CMR).
Background: LV thrombus affects post-MI management. DE-CMR provides thrombus tissue characterization and is a well-validated but an impractical screening modality for all patients after an MI.
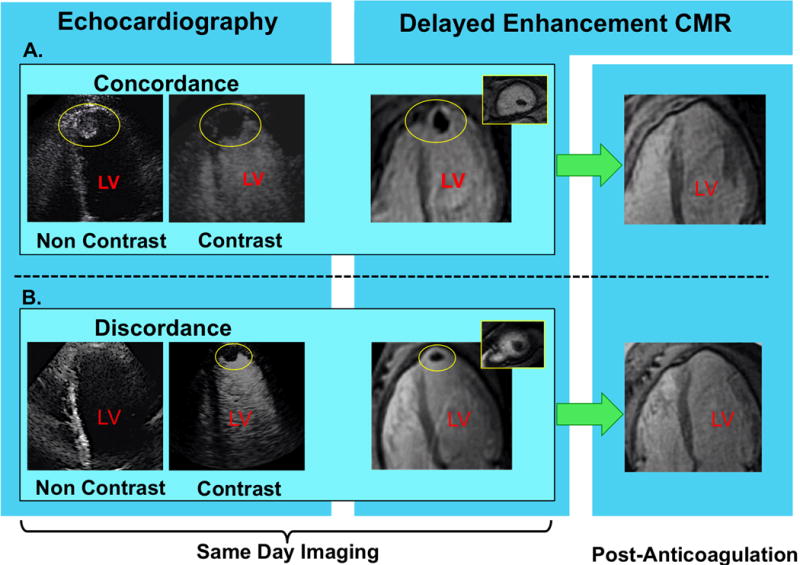
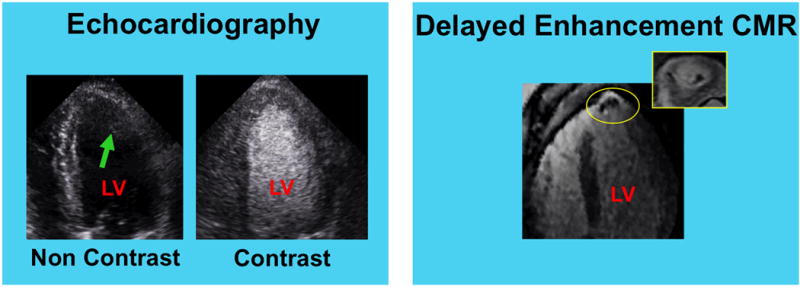
Methods: A same-day echo and CMR were performed according to a tailored protocol, which entailed uniform echo contrast (irrespective of image quality) and dedicated DE-CMR for thrombus tissue characterization.
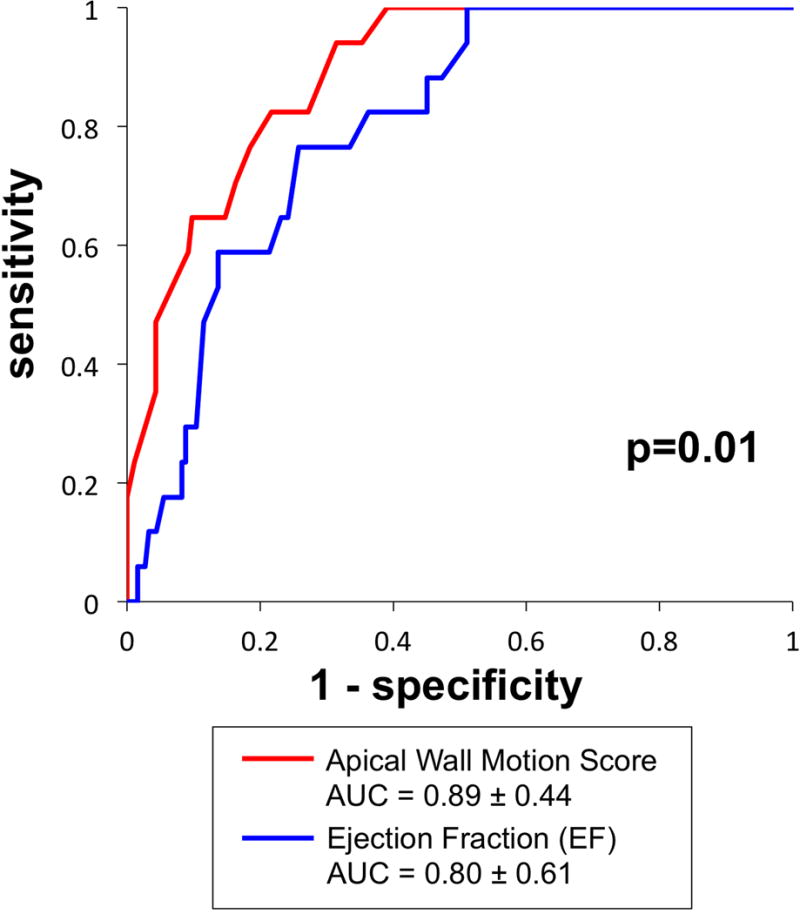
Results: A total of 201 patients were studied; 8% had thrombus according to DE-CMR. All thrombi were apically located; 94% of thrombi occurred in the context of a left anterior descending (LAD) infarct-related artery. Although patients with thrombus had more prolonged chest pain and larger MI (p ≤ 0.01), only 18% had aneurysm on echo (cine-CMR 24%). Noncontrast (35%) and contrast (64%) echo yielded limited sensitivity for thrombus on DE-CMR. Thrombus was associated with stepwise increments in basal → apical contractile dysfunction on echo and quantitative cine-CMR; the echo-measured apical wall motion score was higher among patients with thrombus (p < 0.001) and paralleled cine-CMR decrements in apical ejection fraction and peak ejection rates (both p < 0.005). Thrombus-associated decrements in apical contractile dysfunction were significant even among patients with LAD infarction (p < 0.05). The echo-based apical wall motion score improved overall performance (area under the curve 0.89 ± 0.44) for thrombus compared with ejection fraction (area under the curve 0.80 ± 0.61; p = 0.01). Apical wall motion partitions would have enabled all patients with LV thrombus to be appropriately referred for DE-CMR testing (100% sensitivity and negative predictive value), while avoiding further testing in more than one-half (56% to 63%) of patients.
Conclusions: LV thrombus remains common, especially after LAD MI, and can occur even in the absence of aneurysm. Although DE-CMR yielded improved overall thrombus detection, apical wall motion on a noncontrast echocardiogram can be an effective stratification tool to identify patients in whom DE-CMR thrombus assessment is most warranted. (Diagnostic Utility of Contrast Echocardiography for Detection of LV Thrombi Post ST Elevation Myocardial Infarction; NCT00539045).
Keywords: cardiovascular magnetic resonance; echocardiography; left ventricular thrombus.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interests Disclosure: This work was partially funded through a research grant provided by Lantheus Medical Imaging (echo contrast product manufacturer).
Figures
Comment in
-
Improved Detection by Delayed-Enhancement CMR of LV Thrombus Post-MI: Is This the Answer to Stroke Prevention?JACC Cardiovasc Imaging. 2016 May;9(5):516-8. doi: 10.1016/j.jcmg.2015.07.024. JACC Cardiovasc Imaging. 2016. PMID: 27151520 No abstract available.
References
-
- Mollet NR, Dymarkowski S, Volders W, et al. Visualization of ventricular thrombi with contrast-enhanced magnetic resonance imaging in patients with ischemic heart disease. Circulation. 2002;106:2873–6. - PubMed
-
- Srichai MB, Junor C, Rodriguez LL, et al. Clinical, imaging, and pathologic characteristics of left ventricular thrombus: A comparison of contrast enhanced magnetic resonance imaging, transthoracic echocardiography and transesophageal echocardiography with surgical or pathological validation. American Heart Journal. 2006;152:75–84. - PubMed
-
- Delewi R, Nijveldt R, Hirsch A, et al. Left ventricular thrombus formation after acute myocardial infarction as assessed by cardiovascular magnetic resonance imaging. European journal of radiology. 2012;81:3900–4. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
