

Improving early identification of the high-risk elderly trauma patient by emergency medical services
- PMID: 26477345
- PMCID: PMC4698024
- DOI: 10.1016/j.injury.2015.09.010
Improving early identification of the high-risk elderly trauma patient by emergency medical services
Abstract
Study objective: We sought to (1) define the high-risk elderly trauma patient based on prognostic differences associated with different injury patterns and (2) derive alternative field trauma triage guidelines that mesh with national field triage guidelines to improve identification of high-risk elderly patients.
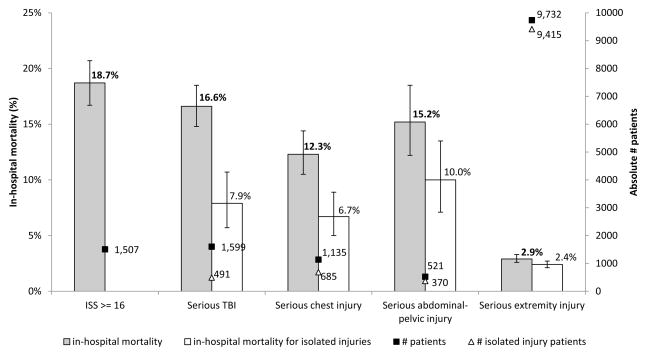
Methods: This was a retrospective cohort study of injured adults ≥65 years transported by 94 EMS agencies to 122 hospitals in 7 regions from 1/1/2006 through 12/31/2008. We tracked current field triage practices by EMS, patient demographics, out-of-hospital physiology, procedures and mechanism of injury. Outcomes included Injury Severity Score≥16 and specific anatomic patterns of serious injury using abbreviated injury scale score ≥3 and surgical interventions. In-hospital mortality was used as a measure of prognosis for different injury patterns.
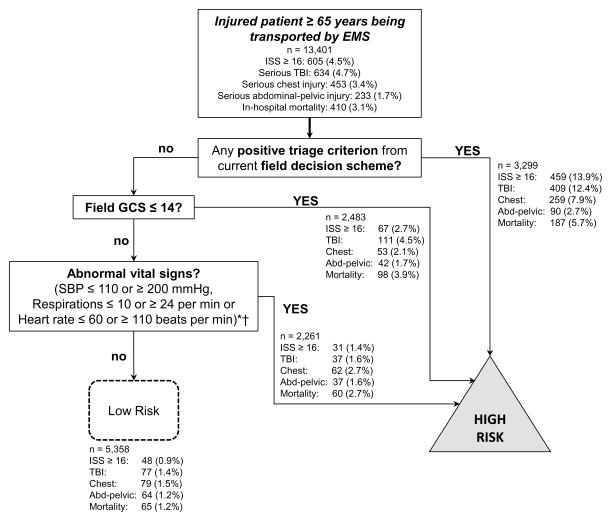
Results: 33,298 injured elderly patients were transported by EMS, including 4.5% with ISS≥16, 4.8% with serious brain injury, 3.4% with serious chest injury, 1.6% with serious abdominal-pelvic injury and 29.2% with serious extremity injury. In-hospital mortality ranged from 18.7% (95% CI 16.7-20.7) for ISS≥16 to 2.9% (95% CI 2.6-3.3) for serious extremity injury. The alternative triage guidelines (any positive criterion from the current guidelines, GCS≤14 or abnormal vital signs) outperformed current field triage practices for identifying patients with ISS≥16: sensitivity (92.1% [95% CI 89.6-94.1%] vs. 75.9% [95% CI 72.3-79.2%]), specificity (41.5% [95% CI 40.6-42.4%] vs. 77.8% [95% CI 77.1-78.5%]). Sensitivity decreased for individual injury patterns, but was higher than current triage practices.
Conclusions: High-risk elderly trauma patients can be defined by ISS≥16 or specific non-extremity injury patterns. The field triage guidelines could be improved to better identify high-risk elderly trauma patients by EMS, with a reduction in triage specificity.
Keywords: Elderly; Emergency medical services; Trauma; Trauma systems; Triage.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
No authors have any financial or personal conflicts of interest that might bias this work.
Figures
References
-
- Wang HE, Mann NC, Jacobson KE, et al. National characteristics of emergency medical services responses in the United States. Prehosp Emerg Care. 2013;17:8–14. - PubMed
-
- Albert MLAJ. NCHS data brief, no 130. Hyattsville, MD: National Center for Health Statistics; 2013. Emergency department visits by persons aged 65 and over: United States, 2009–2010. - PubMed
-
- Newgard C, Zive D, Rea T, et al. A Multi-Site Assessment and Validation of the ACSCOT Trauma Triage Criteria for Identifying Seriously Injured Children and Adults [Abstract] Ann Emerg Med. 2010;56:S28.
-
- Chang DC, Bass RR, Cornwell EE, Mackenzie EJ. Undertriage of elderly trauma patients to state-designated trauma centers. Archives of surgery. 2008;143:776–81. discussion 82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
