Comprehensive Cytomorphologic Analysis of Pulmonary Adenoid Cystic Carcinoma: Comparison to Small Cell Carcinoma and Non-pulmonary Adenoid Cystic Carcinoma
- PMID: 26477588
- PMCID: PMC4696527
- DOI: 10.4132/jptm.2015.09.07
Comprehensive Cytomorphologic Analysis of Pulmonary Adenoid Cystic Carcinoma: Comparison to Small Cell Carcinoma and Non-pulmonary Adenoid Cystic Carcinoma
Abstract
Background: Cytologic diagnosis of pulmonary adenoid cystic carcinoma (AdCC) is frequently challenging and differential diagnosis with small cell carcinoma is often difficult.
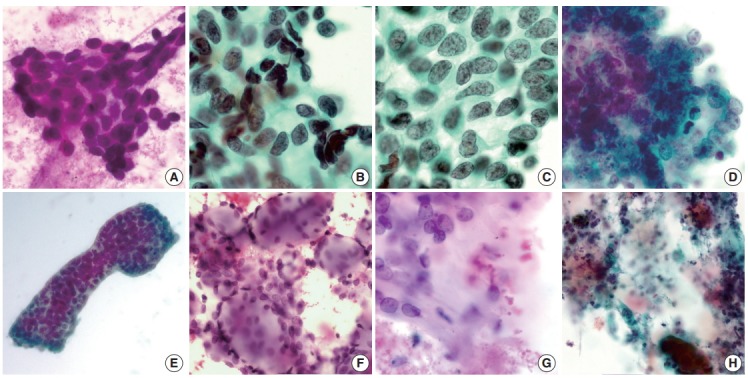
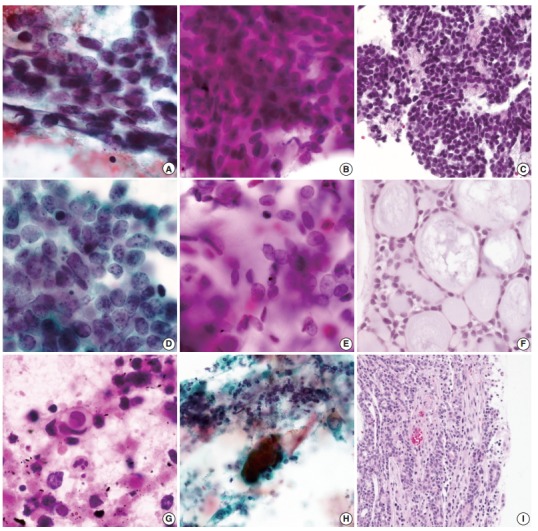
Methods: Eleven cytologically diagnosed cases of pulmonary AdCC were collected and reviewed according to fifteen cytomorphologic characteristics: small cell size, cellular uniformity, coarse chromatin, hyperchromasia, distinct nucleolus, frequent nuclear molding, granular cytoplasm, organoid cluster, sheet formation, irregular border of cluster, hyaline globule, hyaline basement membrane material, individual cell necrosis or apoptotic body, and necrotic background. Twenty cases of small cell carcinoma and fifteen cases of non-pulmonary AdCC were also reviewed for the comparison.
Results: Statistically significant differences were identified between pulmonary AdCC and small cell carcinoma in fourteen of the fifteen cytomorphologic criteria (differences in sheet formation were not statistically significant). Cellular uniformity, distinct nucleolus, granular cytoplasm, distinct cell border, organoid cluster, hyaline globule, and hyaline basement membrane material were characteristic features of AdCC. Frequent nuclear molding, individual cell necrosis, and necrotic background were almost exclusively identified in small cell carcinoma. Although coarse chromatin and irregular cluster border were observed in both, they favored the diagnosis of small cell carcinoma. Hyaline globules were more frequently seen in non-pulmonary AdCC cases.
Conclusions: Using the fifteen cytomorphologic criteria described by this study, pulmonary AdCC could be successfully distinguished from small cell carcinoma. Such a comprehensive approach to an individual case is recommended for the cytologic diagnosis of pulmonary AdCC.
Keywords: Carcinoma, adenoid cystic; Carcinoma, small cell; Cytology; Lung.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
[Cytologic diagnosis of adenoid cystic carcinoma of salivary glands and distinction from basal cell adenoma].Zhonghua Bing Li Xue Za Zhi. 2018 Apr 8;47(4):279-283. doi: 10.3760/cma.j.issn.0529-5807.2018.04.010. Zhonghua Bing Li Xue Za Zhi. 2018. PMID: 29690668 Chinese.
-
A cytodiagnosis of adenoid cystic carcinoma of the tracheobronchial tree through a systematic clinical case comparison and analysis.BMC Pulm Med. 2023 Sep 8;23(1):334. doi: 10.1186/s12890-023-02628-9. BMC Pulm Med. 2023. PMID: 37684618 Free PMC article.
-
Bronchial cytology of pulmonary adenoid cystic carcinoma - A multi-institute series with emphasis on immunocytochemistry.Ann Diagn Pathol. 2023 Jun;64:152132. doi: 10.1016/j.anndiagpath.2023.152132. Epub 2023 Mar 21. Ann Diagn Pathol. 2023. PMID: 36963153
-
Basal cell (monomorphic) and minimally pleomorphic adenomas of the salivary glands. Distinction from the solid (anaplastic) type of adenoid cystic carcinoma in fine-needle aspiration.Am J Clin Pathol. 1996 Jul;106(1):35-41. doi: 10.1093/ajcp/106.1.35. Am J Clin Pathol. 1996. PMID: 8701930 Review.
-
Cervical lymph node metastasis in adenoid cystic carcinoma of oral cavity and oropharynx: A collective international review.Auris Nasus Larynx. 2016 Oct;43(5):477-84. doi: 10.1016/j.anl.2016.02.013. Epub 2016 Mar 24. Auris Nasus Larynx. 2016. PMID: 27017314 Free PMC article. Review.
Cited by
-
Cytology of Primary Salivary Gland-Type Tumors of the Lower Respiratory Tract: Report of 15 Cases and Review of the Literature.Front Med (Lausanne). 2017 Apr 24;4:43. doi: 10.3389/fmed.2017.00043. eCollection 2017. Front Med (Lausanne). 2017. PMID: 28484699 Free PMC article.
-
Pulmonary adenoid cystic carcinoma: molecular characteristics and literature review.Diagn Pathol. 2023 May 17;18(1):65. doi: 10.1186/s13000-023-01354-4. Diagn Pathol. 2023. PMID: 37198615 Free PMC article. Review.
References
-
- Moran CA, Suster S, Koss MN. Primary adenoid cystic carcinoma of the lung: a clinicopathologic and immunohistochemical study of 16 cases. Cancer. 1994;73:1390–7. - PubMed
-
- Maziak DE, Todd TR, Keshavjee SH, Winton TL, Van Nostrand P, Pearson FG. Adenoid cystic carcinoma of the airway: thirty-two-year experience. J Thorac Cardiovasc Surg. 1996;112:1522–31. - PubMed
-
- Cho YM, Park SY, Lee IC. Cytopathologic features of adenoid cystic of trachea carcinoma: report of 2 cases. Korean J Cytopathol. 1995;6:214–8.
-
- Lee JS, Kim JS, Yang BS, Lee MC, Park CS, Juhng SW. Cytopathologic features of primary bronchial adenoid cystic carcinoma: a case report. Korean J Cytopathol. 1995;6:67–70.
LinkOut - more resources
Full Text Sources
Other Literature Sources