

The long-term risk of upper-extremity lymphedema is two-fold higher in breast cancer patients than in melanoma patients
- PMID: 26477877
- PMCID: PMC4715673
- DOI: 10.1002/jso.24068
The long-term risk of upper-extremity lymphedema is two-fold higher in breast cancer patients than in melanoma patients
Abstract
Background and objectives: We assessed the cumulative incidence, symptoms, and risk factors for upper-extremity lymphedema in breast cancer and melanoma patients undergoing sentinel lymph node biopsy or axillary lymph node dissection.
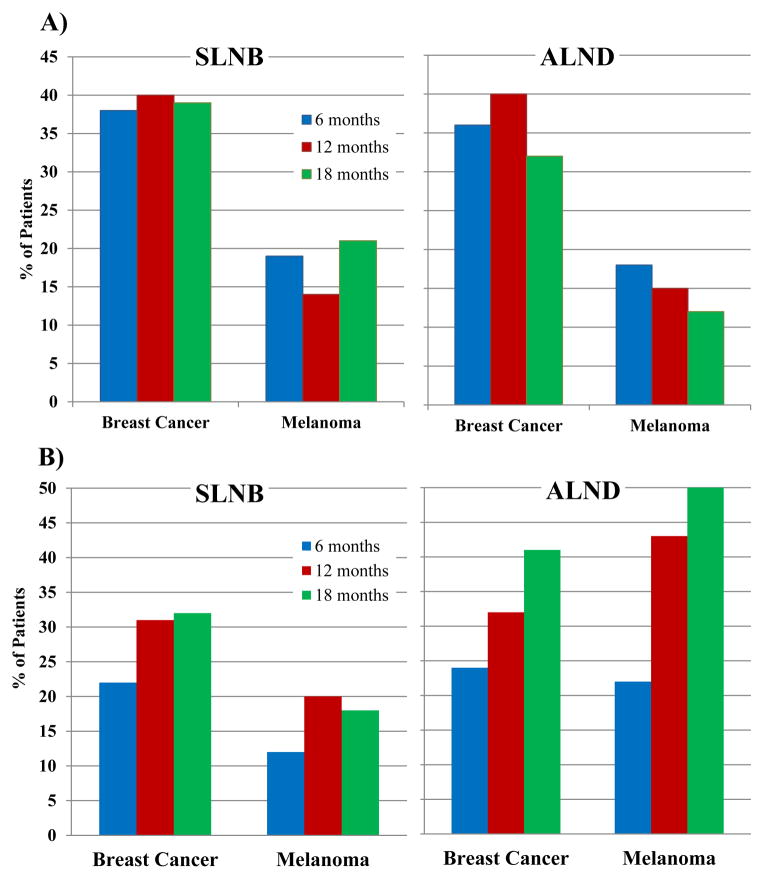
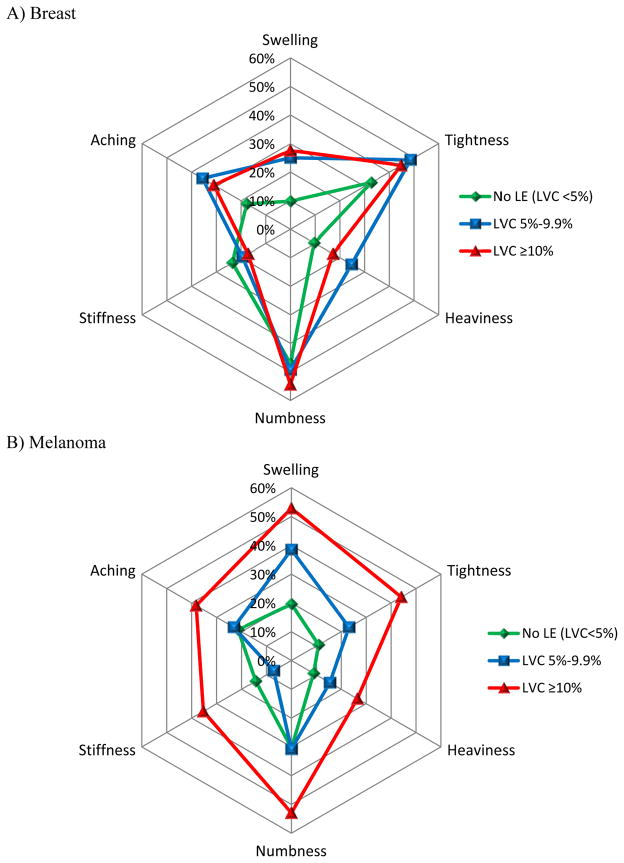
Methods: Patients were recruited preoperatively (time 0) and assessed at 6, 12, and 18 months postoperatively. Limb volume change (LVC) was measured by perometry. Lymphedema was categorized as none, mild (LVC 5-9.9%), or moderate/severe (LVC≥10%). Symptoms were assessed with a validated lymphedema instrument. Longitudinal logistic regression analyses were conducted to identify risk factors associated with moderate/severe lymphedema.
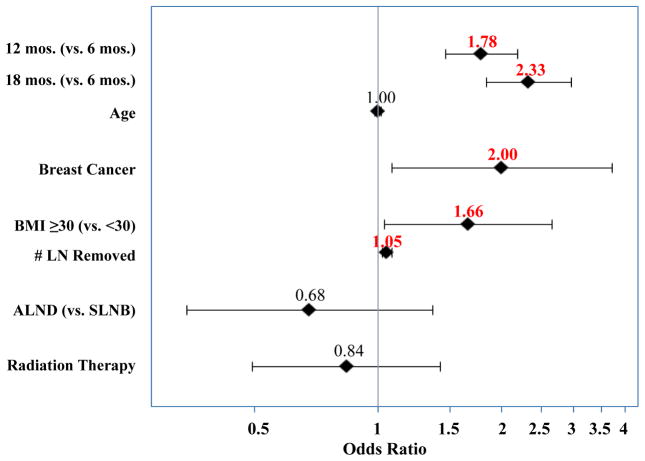
Results: Among 205 breast cancer and 144 melanoma patients, the cumulative incidence of moderate/severe lymphedema at 18 months was 36.5% and 35.0%, respectively. However, in adjusted analyses, factors associated with moderate/severe lymphedema were breast cancer (OR 2.0, P = 0.03), body mass index ≥ 30 kg/m(2) (OR 1.6, P = 0.04), greater number of lymph nodes removed (OR 1.05, P < 0.01), and longer interval since surgery (OR 2.33 at 18 months, P < 0.01).
Conclusions: Lymphedema incidence increased over time in both cohorts. However, the adjusted risk of moderate/severe lymphedema was two-fold higher in breast cancer patients. These results may be attributed to surgical treatment of the primary tumor in the breast and more frequent use of radiation.
Keywords: breast cancer; lymph node excision; lymphedema; melanoma.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65(1):5–29. - PubMed
-
- Cormier JN, et al. Lymphedema beyond breast cancer: a systematic review and meta-analysis of cancer-related secondary lymphedema. Cancer. 2010;116(22):5138–49. - PubMed
-
- de Vries M, et al. Morbidity after axillary sentinel lymph node biopsy in patients with cutaneous melanoma. Eur J Surg Oncol. 2005;31(7):778–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
