

Characterization of IgG4 anti-neurofascin 155 antibody-positive polyneuropathy
- PMID: 26478896
- PMCID: PMC4603379
- DOI: 10.1002/acn3.248
Characterization of IgG4 anti-neurofascin 155 antibody-positive polyneuropathy
Abstract
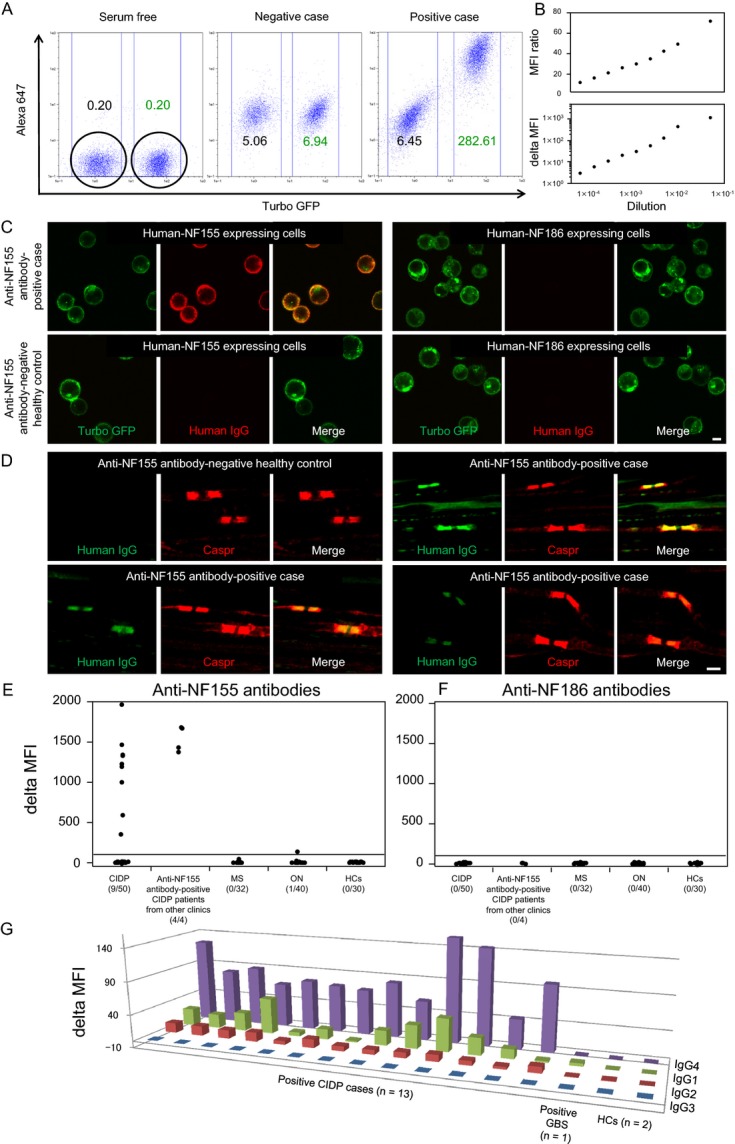
Objective: To investigate anti-neurofascin 155 (NF155) antibody-positive chronic inflammatory demyelinating polyneuropathy (CIDP).
Methods: Sera from 50 consecutive CIDP patients diagnosed in our clinic, 32 patients with multiple sclerosis, 40 patients with other neuropathies including 26 with Guillain-Barré syndrome (GBS)/Fisher syndrome, and 30 healthy controls were measured for anti-NF antibodies by flow cytometry using HEK293 cell lines stably expressing human NF155 or NF186. Four additional CIDP patients with anti-NF155 antibodies referred from other clinics were enrolled for clinical characterization.
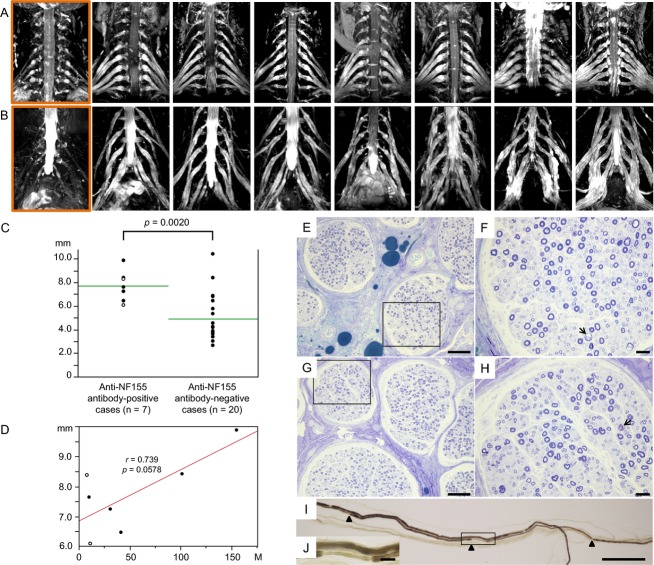
Results: The positivity rate for anti-NF155 antibodies in CIDP patients was 18% (9/50), who all showed a predominance of IgG4 subclass. No other subjects were positive, except one GBS patient harboring IgG1 anti-NF155 antibodies. No anti-NF155 antibody carriers had anti-NF186 antibodies. Anti-NF155 antibody-positive CIDP patients had a significantly younger onset age, higher frequency of drop foot, gait disturbance, tremor and distal acquired demyelinating symmetric phenotype, greater cervical root diameter on magnetic resonance imaging neurography, higher cerebrospinal fluid protein levels, and longer distal and F-wave latencies than anti-NF155 antibody-negative patients. Marked symmetric hypertrophy of cervical and lumbosacral roots/plexuses was present in all anti-NF155 antibody-positive CIDP patients examined by neurography. Biopsied sural nerves from two patients with anti-NF155 antibodies demonstrated subperineurial edema and occasional paranodal demyelination, but no vasculitis, inflammatory cell infiltrates, or onion bulbs. Among anti-NF155 antibody-positive patients, treatment responders more frequently had daily oral corticosteroids and/or immunosuppressants in addition to intravenous immunoglobulins than nonresponders did.
Interpretation: Anti-NF155 antibodies occur in a subset of CIDP patients with distal-dominant involvement and symmetric nerve hypertrophy.
Figures
References
-
- Dalakas MC. Advances in the diagnosis, pathogenesis and treatment of CIDP. Nat Rev Neurol. 2011;7:507–517. - PubMed
-
- Querol L, Nogales-Gadea G, Rojas-Garcia R, et al. Antibodies to contactin-1 in chronic inflammatory demyelinating polyneuropathy. Ann Neurol. 2013;73:370–380. - PubMed
-
- Sherman DL, Tait S, Melrose S, et al. Neurofascins are required to establish axonal domains for saltatory conduction. Neuron. 2005;48:737–742. - PubMed
-
- Pedraza L, Huang JK, Colman DR. Organizing principles of the axoglial apparatus. Neuron. 2001;30:335–344. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
