

Effect of health risk assessment and counselling on health behaviour and survival in older people: a pragmatic randomised trial
- PMID: 26479077
- PMCID: PMC4610679
- DOI: 10.1371/journal.pmed.1001889
Effect of health risk assessment and counselling on health behaviour and survival in older people: a pragmatic randomised trial
Abstract
Background: Potentially avoidable risk factors continue to cause unnecessary disability and premature death in older people. Health risk assessment (HRA), a method successfully used in working-age populations, is a promising method for cost-effective health promotion and preventive care in older individuals, but the long-term effects of this approach are unknown. The objective of this study was to evaluate the effects of an innovative approach to HRA and counselling in older individuals for health behaviours, preventive care, and long-term survival.
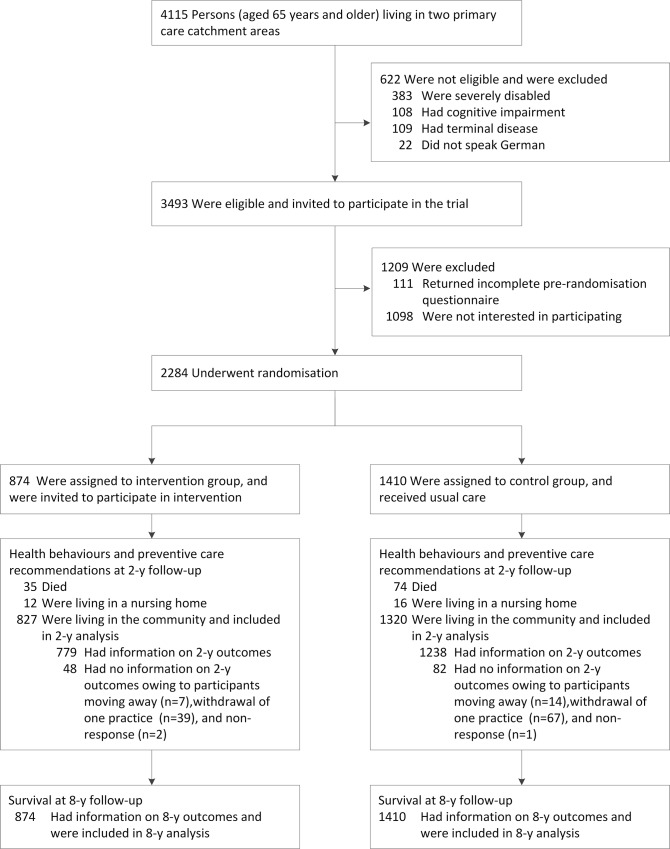
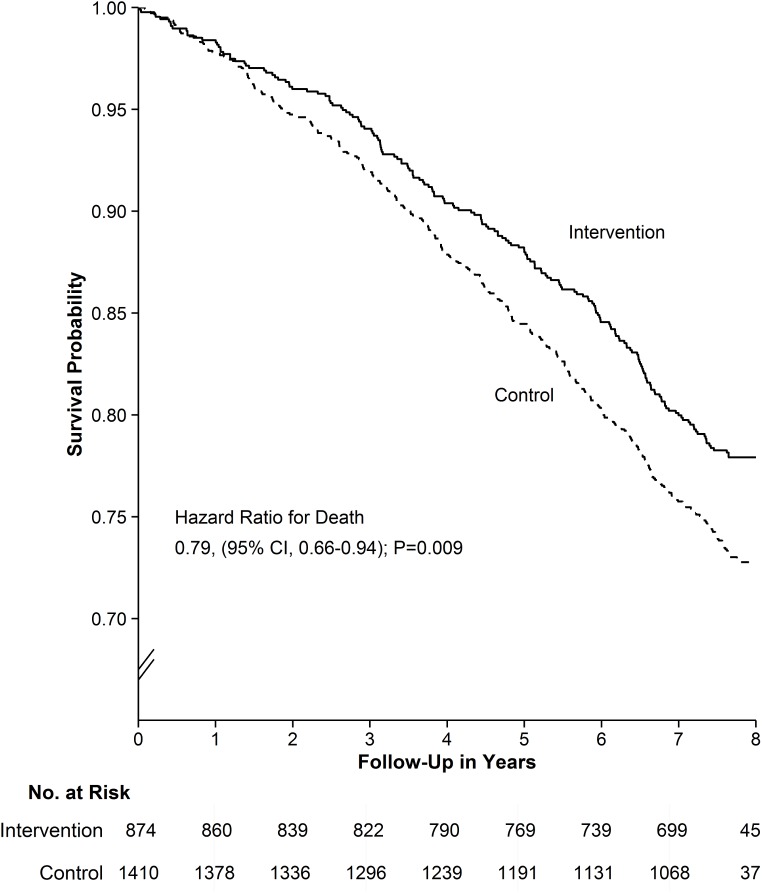
Methods and findings: This study was a pragmatic, single-centre randomised controlled clinical trial in community-dwelling individuals aged 65 y or older registered with one of 19 primary care physician (PCP) practices in a mixed rural and urban area in Switzerland. From November 2000 to January 2002, 874 participants were randomly allocated to the intervention and 1,410 to usual care. The intervention consisted of HRA based on self-administered questionnaires and individualised computer-generated feedback reports, combined with nurse and PCP counselling over a 2-y period. Primary outcomes were health behaviours and preventive care use at 2 y and all-cause mortality at 8 y. At baseline, participants in the intervention group had a mean ± standard deviation of 6.9 ± 3.7 risk factors (including unfavourable health behaviours, health and functional impairments, and social risk factors) and 4.3 ± 1.8 deficits in recommended preventive care. At 2 y, favourable health behaviours and use of preventive care were more frequent in the intervention than in the control group (based on z-statistics from generalised estimating equation models). For example, 70% compared to 62% were physically active (odds ratio 1.43, 95% CI 1.16-1.77, p = 0.001), and 66% compared to 59% had influenza vaccinations in the past year (odds ratio 1.35, 95% CI 1.09-1.66, p = 0.005). At 8 y, based on an intention-to-treat analysis, the estimated proportion alive was 77.9% in the intervention and 72.8% in the control group, for an absolute mortality difference of 4.9% (95% CI 1.3%-8.5%, p = 0.009; based on z-test for risk difference). The hazard ratio of death comparing intervention with control was 0.79 (95% CI 0.66-0.94, p = 0.009; based on Wald test from Cox regression model), and the number needed to receive the intervention to prevent one death was 21 (95% CI 12-79). The main limitations of the study include the single-site study design, the use of a brief self-administered questionnaire for 2-y outcome data collection, the unavailability of other long-term outcome data (e.g., functional status, nursing home admissions), and the availability of long-term follow-up data on mortality for analysis only in 2014.
Conclusions: This is the first trial to our knowledge demonstrating that a collaborative care model of HRA in community-dwelling older people not only results in better health behaviours and increased use of recommended preventive care interventions, but also improves survival. The intervention tested in our study may serve as a model of how to implement a relatively low-cost but effective programme of disease prevention and health promotion in older individuals.
Trial registration: International Standard Randomized Controlled Trial Number: ISRCTN 28458424.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–2260. - PMC - PubMed
-
- National Center for Chronic Disease Prevention and Health Promotion. The state of aging and health in America 2013. US Department of Health and Human Services; 2013. Available: http://www.cdc.gov/aging/pdf/state-aging-health-in-america-2013.pdf. Accessed August 31, 2015.
-
- National Institute on Aging, World Health Organization. Global health and aging. Geneva: World Health Organization; 2011. Available: http://www.who.int/ageing/publications/global_health.pdf. Accessed August 31, 2015.
-
- Krogsbøll LT, Jørgensen KJ, Gøtzsche PC. General health checks in adults for reducing morbidity and mortality from disease. JAMA. 2013;309:2489–2490. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
