

Long-term survival and T-cell kinetics in relapsed/refractory ALL patients who achieved MRD response after blinatumomab treatment
- PMID: 26480933
- PMCID: PMC4671107
- DOI: 10.1182/blood-2015-06-649111
Long-term survival and T-cell kinetics in relapsed/refractory ALL patients who achieved MRD response after blinatumomab treatment
Abstract
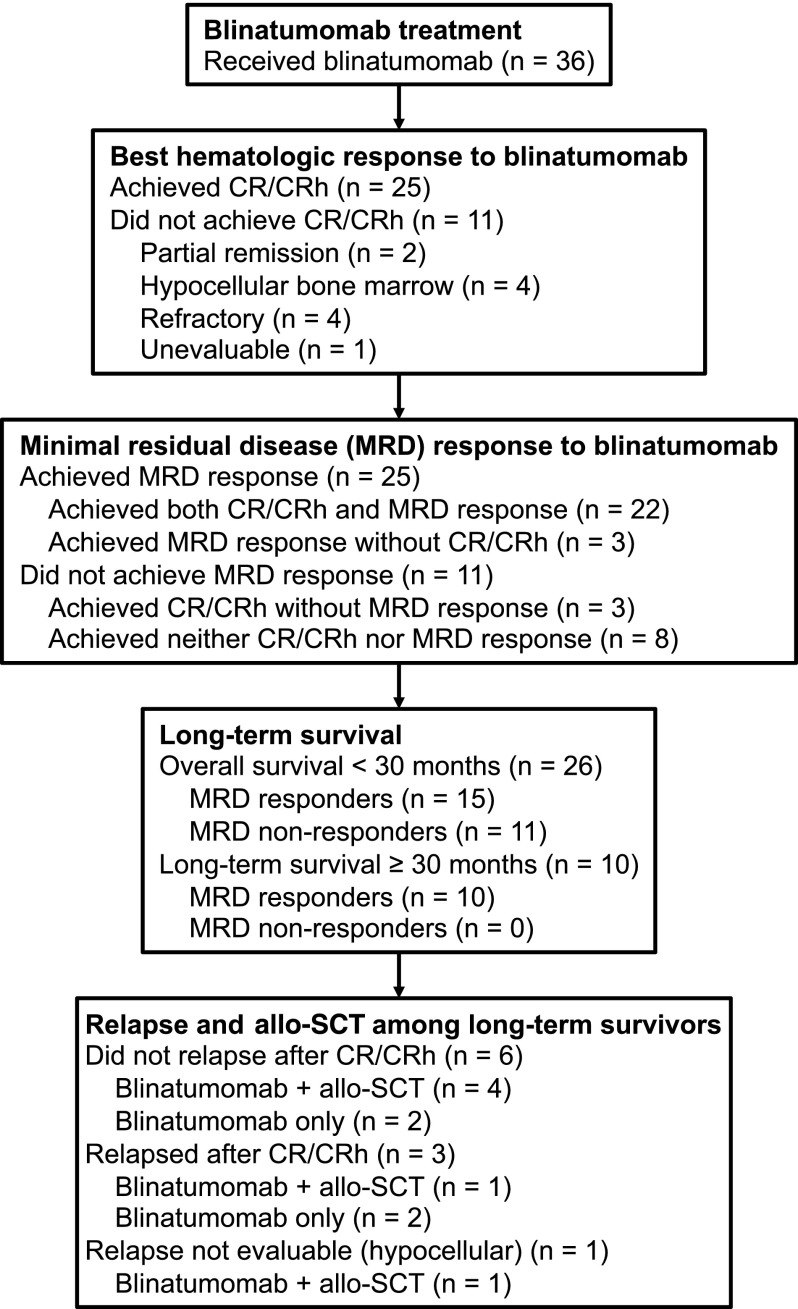
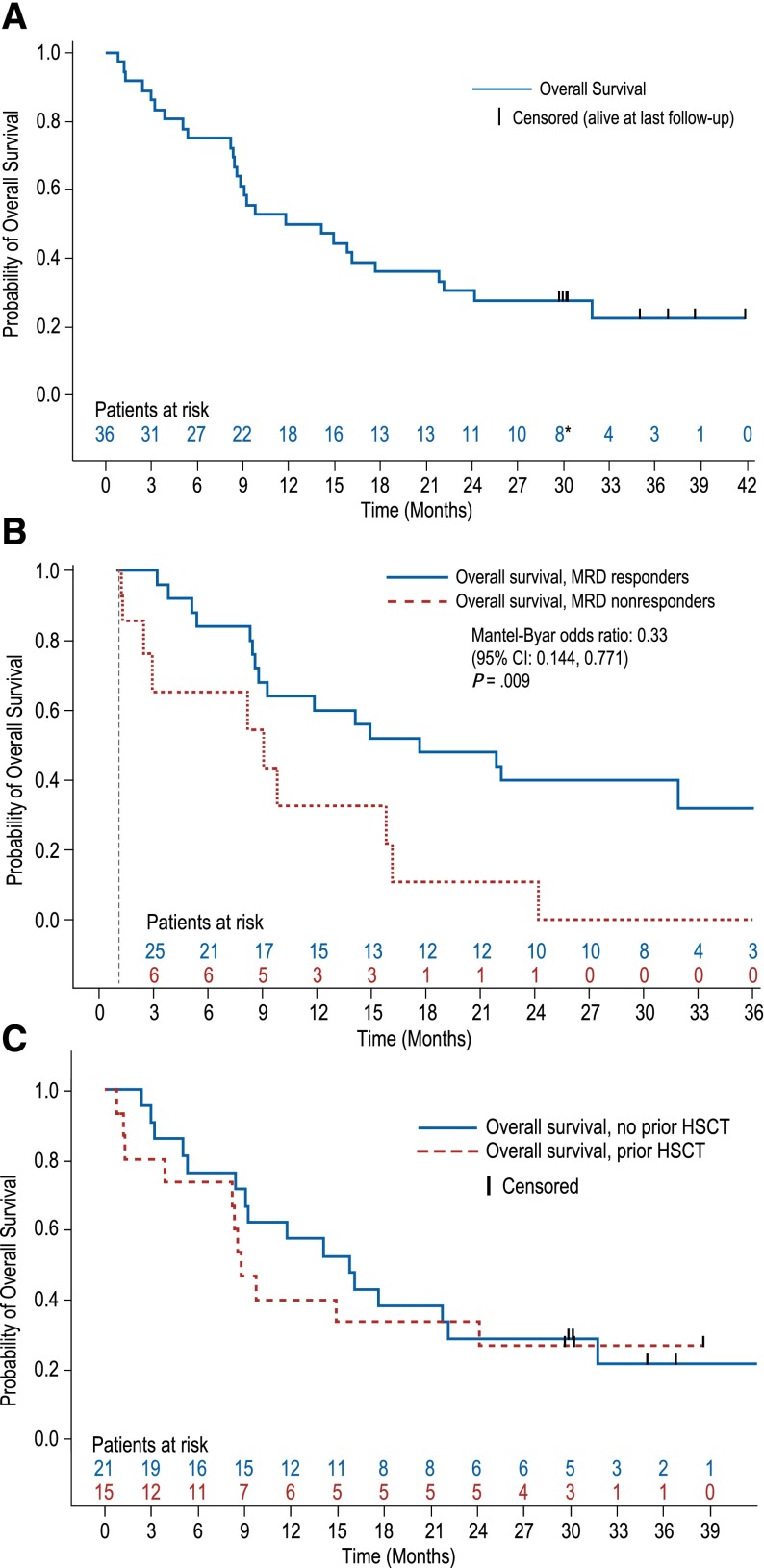
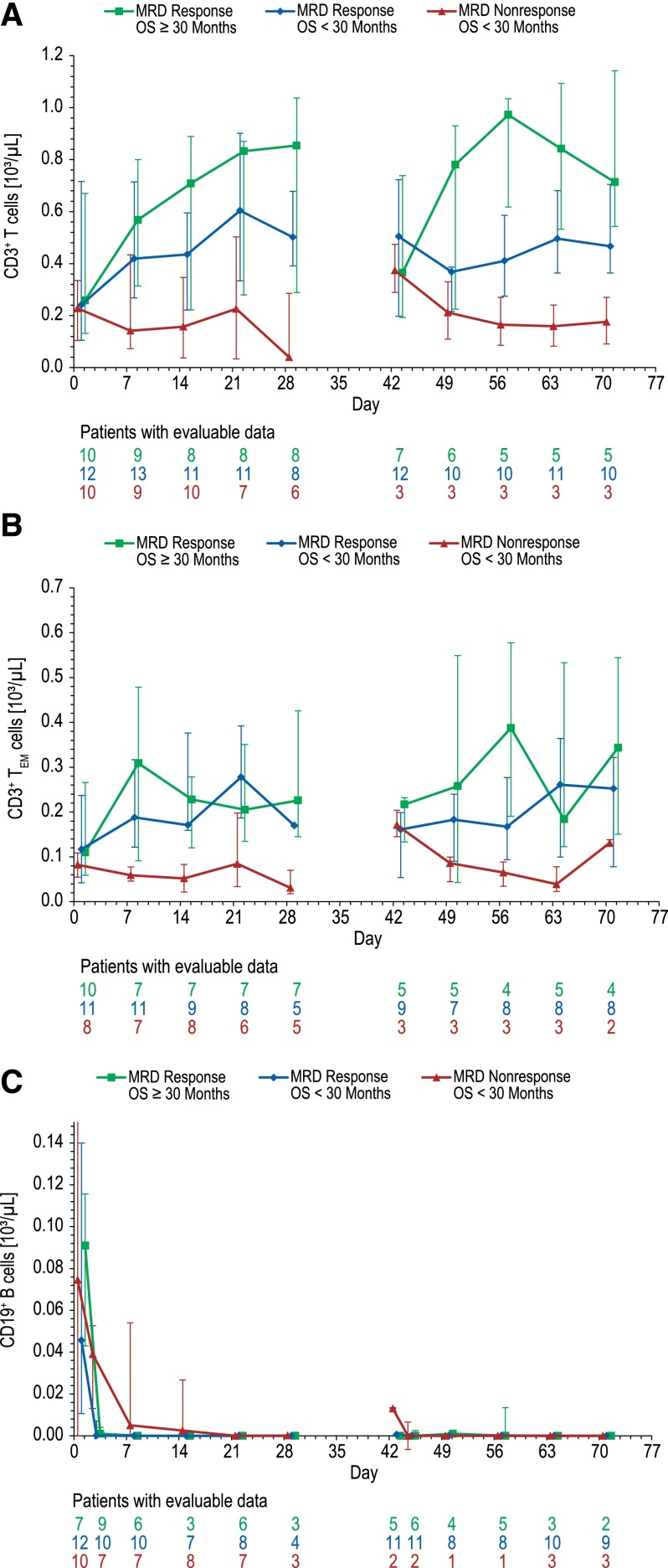
This long-term follow-up analysis evaluated overall survival (OS) and relapse-free survival (RFS) in a phase 2 study of the bispecific T-cell engager antibody construct blinatumomab in 36 adults with relapsed/refractory B-precursor acute lymphoblastic leukemia (ALL). In the primary analysis, 25 (69%) patients with relapsed/refractory ALL achieved complete remission with full (CR) or partial (CRh) hematologic recovery of peripheral blood counts within the first 2 cycles. Twenty-five patients (69%) had a minimal residual disease (MRD) response (<10(-4) blasts), including 22 CR/CRh responders, 2 patients with hypocellular bone marrow, and 1 patient with normocellular bone marrow but low peripheral counts. Ten of the 36 patients (28%) were long-term survivors (OS ≥30 months). Median OS was 13.0 months (median follow-up, 32.6 months). MRD response was associated with significantly longer OS (Mantel-Byar P = .009). All 10 long-term survivors had an MRD response. Median RFS was 8.8 months (median follow-up, 28.9 months). A plateau for RFS was reached after ∼18 months. Six of the 10 long-term survivors remained relapse-free, including 4 who received allogeneic stem cell transplantation (allo-SCT) as consolidation for blinatumomab and 2 who received 3 additional cycles of blinatumomab instead of allo-SCT. Three long-term survivors had neurologic events or cytokine release syndrome, resulting in temporary blinatumomab discontinuation; all restarted blinatumomab successfully. Long-term survivors had more pronounced T-cell expansion than patients with OS <30 months.
© 2015 by The American Society of Hematology.
Figures

References
-
- Tavernier E, Boiron JM, Huguet F, et al. GET-LALA Group; Swiss Group for Clinical Cancer Research SAKK; Australasian Leukaemia and Lymphoma Group. Outcome of treatment after first relapse in adults with acute lymphoblastic leukemia initially treated by the LALA-94 trial. Leukemia. 2007;21(9):1907–1914. - PubMed
-
- Fielding AK, Richards SM, Chopra R, et al. Medical Research Council of the United Kingdom Adult ALL Working Party; Eastern Cooperative Oncology Group. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2007;109(3):944–950. - PubMed
-
- Gökbuget N, Stanze D, Beck J, et al. German Multicenter Study Group for Adult Acute Lymphoblastic Leukemia. Outcome of relapsed adult lymphoblastic leukemia depends on response to salvage chemotherapy, prognostic factors, and performance of stem cell transplantation. Blood. 2012;120(10):2032–2041. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
