

Increase in Disability Prevalence Before Hip Fracture
- PMID: 26480970
- PMCID: PMC4699653
- DOI: 10.1111/jgs.13658
Increase in Disability Prevalence Before Hip Fracture
Abstract
Objectives: To establish the prevalence and correlates of disability during the 2 years before hip fracture.
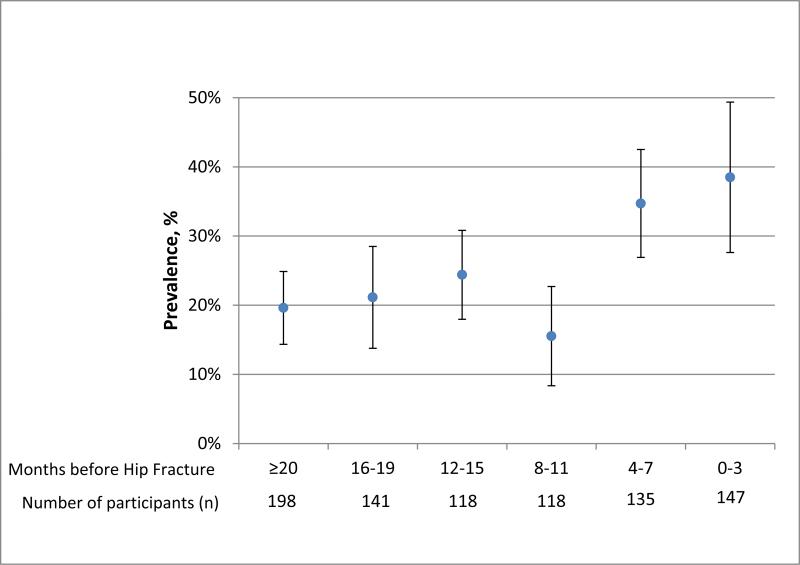
Design: Data from participants who experienced hip fracture in the Health and Retirement Study (HRS) with hip fracture identified using linked Medicare claims. Each participant was interviewed at varying time points in the 2 years before hip fracture. Disability was defined as self-report of the need for assistance in any activity of daily living (walking across the room, eating, bathing, dressing, using the toilet, transferring). Based on the timing between interview and hip fracture, prevalence of disability was calculated in the cohort as a whole over the 2 years before hip fracture and in subgroups defined according to demographic and clinical characteristics.
Setting: The HRS is a nationally representative longitudinal study (1992-2010).
Participants: HRS participants aged ≥65 with hip fracture (mean age at fracture 84, 77% female).
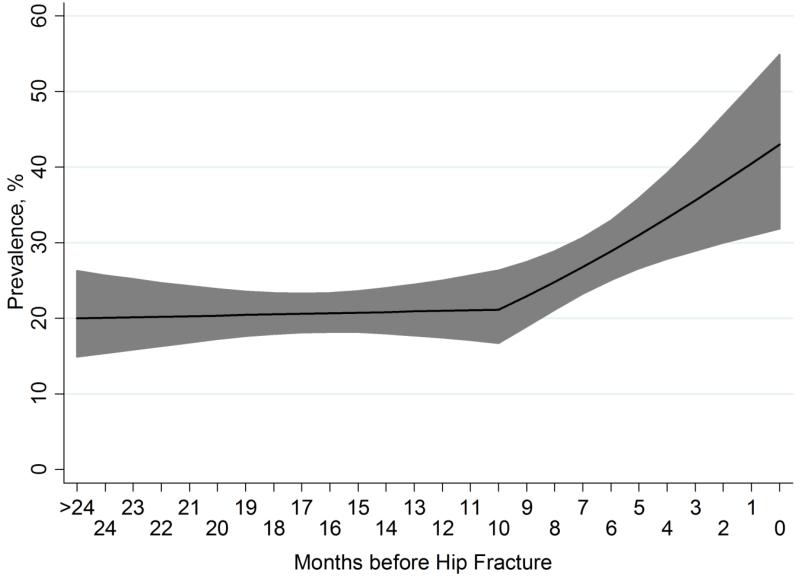
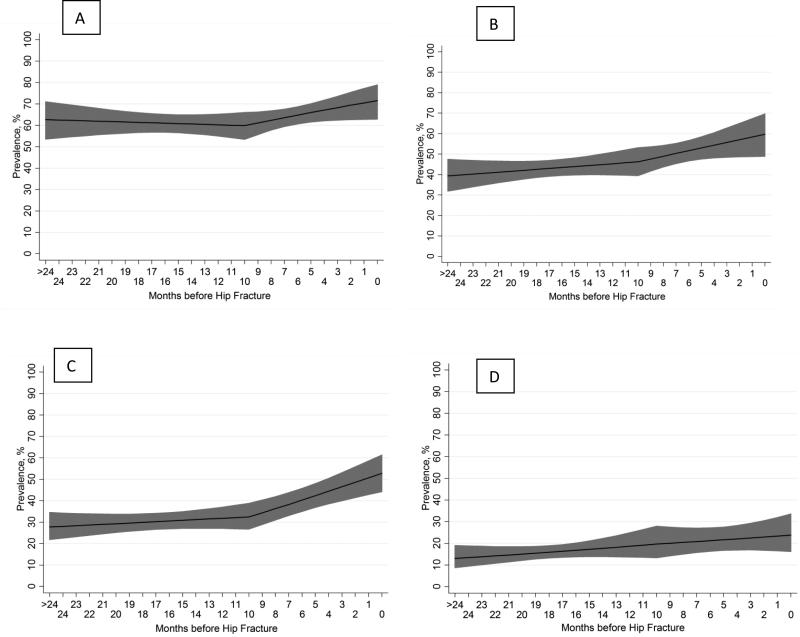
Results: The adjusted prevalence of disability was 20% (95% confidence interval (CI) = 14-25%) 2 years before hip fracture, with little change until approximately 10 months before fracture, when it started to rise, reaching 44% (95% CI = 33-55%) in the month before hip fracture. The prevalence of disability was highest in the last month before fracture for persons aged 85 and older (53%) and for those with dementia (60%).
Conclusion: Care models for hip fracture need to consider not only the acute medical and surgical needs, but also the high level of need for supportive care and caregiver assistance that chronically disabled individuals require.
Keywords: disability; epidemiology; hip fracture.
© 2015, Copyright the Authors Journal compilation © 2015, The American Geriatrics Society.
Figures
References
-
- [March 28, 2014];Hospital discharges by first- and any-listed diagnosis: US, 1990-2010 (Source: NHDS) 2010 http://205.207.175.93/HDI/TableViewer/tableView.aspx. 2014.
-
- Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 1997;7(5):407–413. - PubMed
-
- Magaziner J, Hawkes W, Hebel JR, et al. Recovery from hip fracture in eight areas of function. The journals of gerontology. Series A, Biological sciences and medical sciences. 2000 Sep;55(9):M498–507. - PubMed
-
- Magaziner J, Simonsick EM, Kashner TM, Hebel JR, Kenzora JE. Predictors of functional recovery one year following hospital discharge for hip fracture: a prospective study. Journal of gerontology. 1990 May;45(3):M101–107. - PubMed
-
- Magaziner J, Fredman L, Hawkes W, et al. Changes in functional status attributable to hip fracture: a comparison of hip fracture patients to community-dwelling aged. American journal of epidemiology. 2003 Jun 1;157(11):1023–1031. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
