

Face and content validity of a virtual-reality simulator for myringotomy with tube placement
- PMID: 26481401
- PMCID: PMC4615336
- DOI: 10.1186/s40463-015-0094-2
Face and content validity of a virtual-reality simulator for myringotomy with tube placement
Abstract
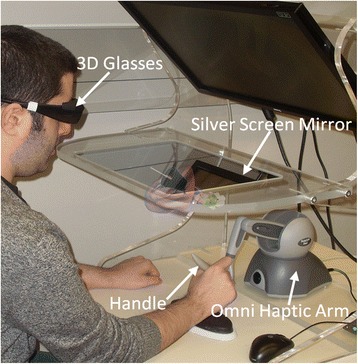
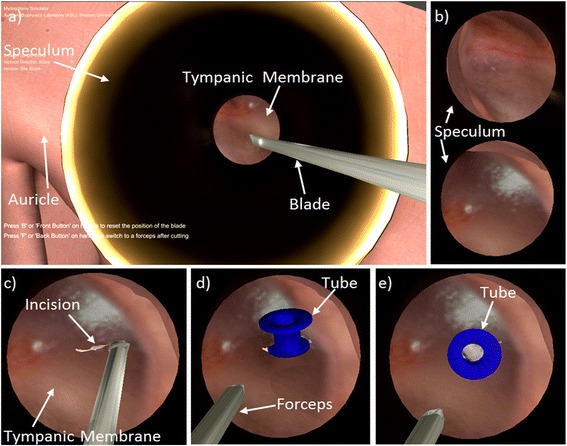
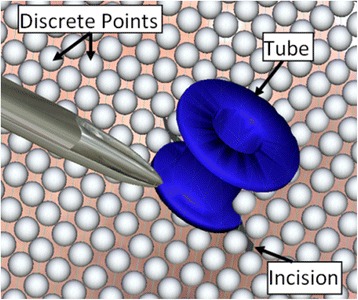
Background: Myringotomy with tube insertion can be challenging for junior Otolaryngology residents as it is one of the first microscopic procedures they encounter. The Western myringotomy simulator was developed to allow trainees to practice microscope positioning, myringotomy, and tube placement. This virtual-reality simulator is viewed in stereoscopic 3D, and a haptic device is used to manipulate the digital ear model and surgical tools.
Objective: To assess the face and content validity of the Western myringotomy simulator.
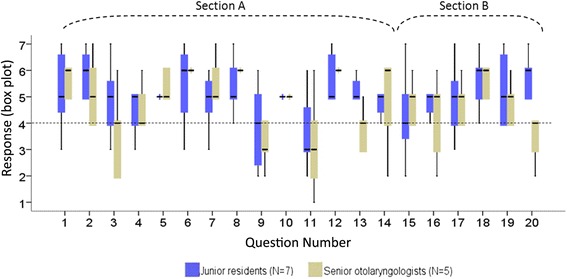
Methods: The myringotomy simulator was integrated with new modules to allow speculum placement, manipulation of an operative microscope, and insertion of the ventilation tube through a deformable tympanic membrane. A questionnaire was developed in consultation with instructing surgeons. Fourteen face validity questions focused on the anatomy of the ear, simulation of the operative microscope, appearance and movement of the surgical instruments, deformation and cutting of the eardrum, and myringotomy tube insertion. Six content validity questions focused on training potential on surgical tasks such as speculum placement, microscope positioning, tool navigation, ear anatomy, myringotomy creation and tube insertion. A total of 12 participants from the Department of Otolaryngology-Head and Neck Surgery were recruited for the study. Prior to completing the questionnaire, participants were oriented to the simulator and given unlimited time to practice until they were comfortable with all of its aspects.
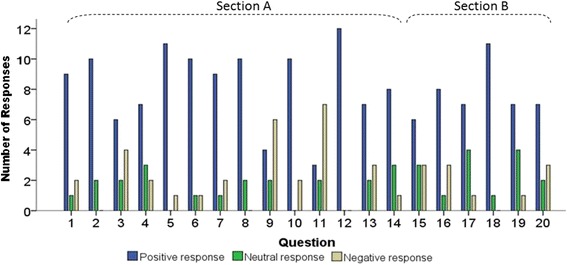
Results: Responses to 12 of the 14 questions on face validity were predominantly positive. One issue of concern was with contact modeling related to tube insertion into the eardrum, and the second was with the movement of the blade and forceps. The former could be resolved by using a higher resolution digital model for the eardrum to improve contact localization. The latter could be resolved by using a higher fidelity haptic device. With regard to content validity, 64% of the responses were positive, 21% were neutral, and 15% were negative.
Conclusions: The Western myringotomy simulator appears to have sufficient face and content validity. Further development with automated metrics and skills transference testing is planned.
Figures
Similar articles
-
Virtual reality myringotomy simulation with real-time deformation: development and validity testing.Laryngoscope. 2012 Aug;122(8):1844-51. doi: 10.1002/lary.23361. Epub 2012 May 7. Laryngoscope. 2012. PMID: 22566189
-
Development and face validity testing of a three-dimensional myringotomy simulator with haptic feedback.J Otolaryngol Head Neck Surg. 2010 Apr;39(2):122-9. J Otolaryngol Head Neck Surg. 2010. PMID: 20211097
-
Interactive computer-based simulator for training in blade navigation and targeting in myringotomy.Comput Methods Programs Biomed. 2010 May;98(2):130-9. doi: 10.1016/j.cmpb.2009.09.010. Epub 2009 Oct 24. Comput Methods Programs Biomed. 2010. PMID: 19854532
-
Automated Metrics in a Virtual-Reality Myringotomy Simulator: Development and Construct Validity.Otol Neurotol. 2018 Aug;39(7):e601-e608. doi: 10.1097/MAO.0000000000001867. Otol Neurotol. 2018. PMID: 29912829
-
Physical Models and Virtual Reality Simulators in Otolaryngology.Otolaryngol Clin North Am. 2017 Oct;50(5):875-891. doi: 10.1016/j.otc.2017.05.001. Epub 2017 Jul 14. Otolaryngol Clin North Am. 2017. PMID: 28716337 Review.
Cited by
-
How I do it: a simulator of the ear for developing otomicroscopy skills during the coronavirus disease 2019 pandemic.J Laryngol Otol. 2020 Oct 21:1-4. doi: 10.1017/S0022215120002261. Online ahead of print. J Laryngol Otol. 2020. PMID: 33081871 Free PMC article.
-
Assessment of a virtual reality temporal bone surgical simulator: a national face and content validity study.J Otolaryngol Head Neck Surg. 2020 Apr 7;49(1):17. doi: 10.1186/s40463-020-00411-y. J Otolaryngol Head Neck Surg. 2020. PMID: 32264952 Free PMC article.
-
The Opportunities and Challenges of Digital Anatomy for Medical Sciences: Narrative Review.JMIR Med Educ. 2022 May 20;8(2):e34687. doi: 10.2196/34687. JMIR Med Educ. 2022. PMID: 35594064 Free PMC article. Review.
-
A modular surgical simulator for microlaryngoscopy using standard instruments and the carbon dioxide laser.Laryngoscope Investig Otolaryngol. 2022 Jun 30;7(4):1065-1070. doi: 10.1002/lio2.854. eCollection 2022 Aug. Laryngoscope Investig Otolaryngol. 2022. PMID: 36000063 Free PMC article.
-
Otologic Skills Training.Otolaryngol Clin North Am. 2017 Oct;50(5):933-945. doi: 10.1016/j.otc.2017.05.005. Epub 2017 Aug 16. Otolaryngol Clin North Am. 2017. PMID: 28822580 Free PMC article. Review.
References
-
- Kumar M, Khan AM, Davis S. Medial displacement of grommets: an unwanted sequel of grommet insertion. J Laryngol Otol. 2000;114:448–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
