

Pitfalls in the Use of Stereoacuity in the Diagnosis of Nonorganic Visual Loss
- PMID: 26481817
- PMCID: PMC4695302
- DOI: 10.1016/j.ophtha.2015.09.024
Pitfalls in the Use of Stereoacuity in the Diagnosis of Nonorganic Visual Loss
Abstract
Purpose: The Titmus Stereotest (Stereo Optical Co., Inc., Chicago, IL) has been used to estimate visual acuity (VA) in the evaluation of nonorganic visual loss. Previous predictions were derived from optical degradation of VA in normal subjects and may not account for the variability seen in patients with neuro-ophthalmic pathologies included in the differential diagnosis of nonorganic visual loss. The purpose of this study was to evaluate the relationship between Titmus stereoacuity and minimal VA based on a real-world testing environment.
Design: Cross-sectional observational study.
Participants: All patients treated at the authors' neuro-ophthalmology service between April 25, 2014, and July 31, 2014.
Methods: All subjects underwent routine neuro-ophthalmic examination, including Titmus stereoacuity measurements. A compound Bayesian logit-lognormal model accounting for heteroscedasticity was used to determine 95% and 99% prediction intervals of the worse eye's near VA based on stereoacuity. Logarithm of the minimum angle of resolution VA and log stereoacuity were analyzed.
Main outcome measures: Titmus stereoacuity and worse eye VA.
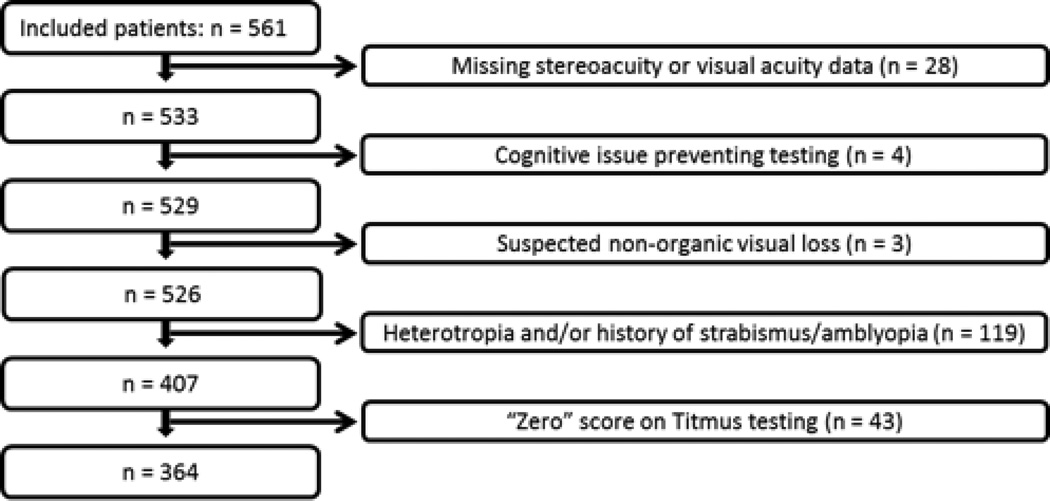
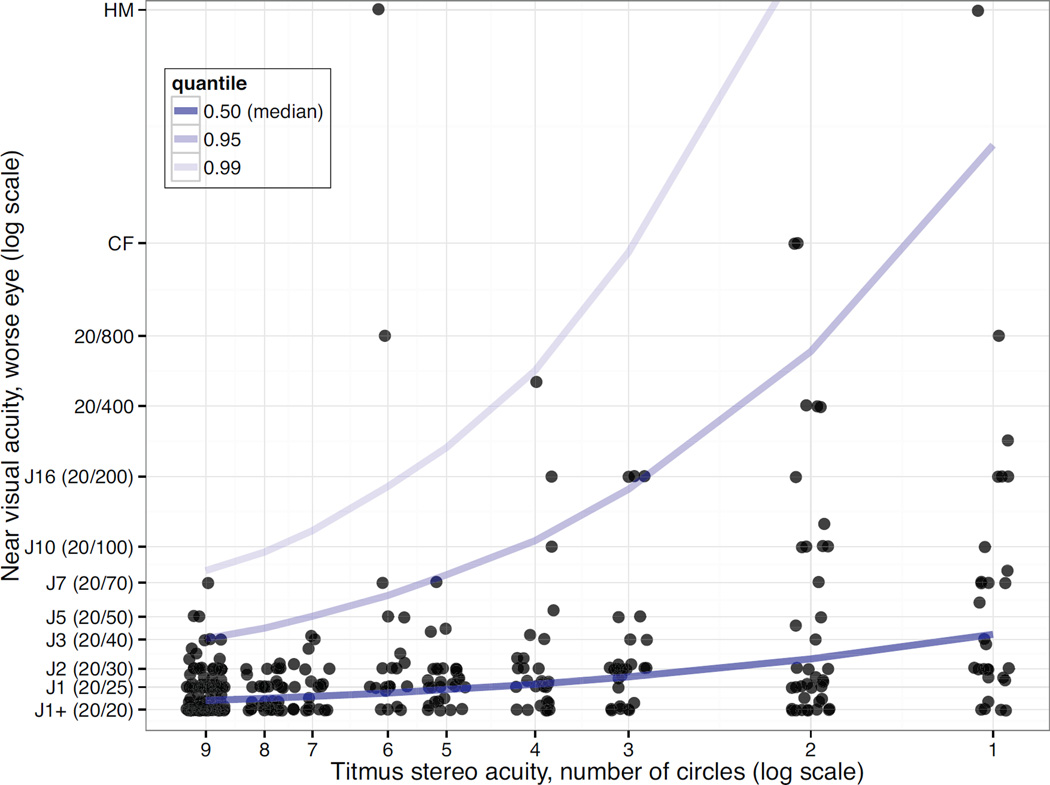
Results: Of 561 patients, 364 subjects 11 to 91 years of age were included. Titmus stereoacuity was associated positively with VA: 9 circles correct (40 seconds of arc) indicated VA of at least 20/40 with 95% confidence and VA of at least 20/79 with 99% confidence; 6 circles correct (80 seconds of arc) indicated VA of at least 20/62 and 20/180, respectively; and 4 circles correct (140 seconds of arc) indicated VA of at least 20/110 and 20/570, respectively.
Conclusions: When fully accounting for individual variation and the full spectrum of neuro-ophthalmic diseases affecting VA, stereoacuity remains associated with VA, but previous commonly used VA estimates based on stereoacuity overestimated VA. Our results more accurately predict minimum VA from Titmus stereoacuity and should be used preferentially when evaluating patients with suspected nonorganic visual loss. We demonstrated that Titmus stereoacuity cannot definitively establish normal VA, and therefore can suggest, but not fully establish, the diagnosis of nonorganic visual loss.
Copyright © 2016 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: The authors have no proprietary or commercial interest in any materials discussed in this article
Figures
Comment in
-
Re: Sitko et al.: Pitfalls in the use of stereoacuity in the diagnosis of nonorganic visual loss (Ophthalmology 2016;123:198-202).Ophthalmology. 2016 Aug;123(8):e47. doi: 10.1016/j.ophtha.2016.01.054. Ophthalmology. 2016. PMID: 27450822 No abstract available.
-
Reply.Ophthalmology. 2016 Aug;123(8):e47. doi: 10.1016/j.ophtha.2016.02.004. Ophthalmology. 2016. PMID: 27450823 No abstract available.
References
-
- Stigmar G. Blurred visual stimuli II: The effect of blurred visual stimuli on Vernier and stereo acuity. Act Ophthalmol. 1971;49:364–379. - PubMed
-
- Berry RN. Quantitative relations among Vernier, real depth, and stereoscopic depth acuities. J Exp Psychol. 1948;38:708–721. - PubMed
-
- Geib T, Baumann C. Effect of luminance and contrast on stereoscopic acuity. Graefes Arch Clin Exp Ophthalmol. 1990;228:310–315. - PubMed
-
- Westheimer G, Pettet MW. Contrast and duration of exposure differentially affect Vernier and stereoscopic acuity. Proc R Soc Lond B. 1990;241:42–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
