

BP and Renal Outcomes in Diabetic Kidney Disease: The Veterans Affairs Nephropathy in Diabetes Trial
- PMID: 26482258
- PMCID: PMC4670761
- DOI: 10.2215/CJN.02850315
BP and Renal Outcomes in Diabetic Kidney Disease: The Veterans Affairs Nephropathy in Diabetes Trial
Abstract
Background and objectives: Proteinuric diabetic kidney disease frequently progresses to ESRD. Control of BP delays progression, but the optimal BP to improve outcomes remains unclear. The objective of this analysis was to evaluate the relationship between BP and renal outcomes in proteinuric diabetic kidney disease.
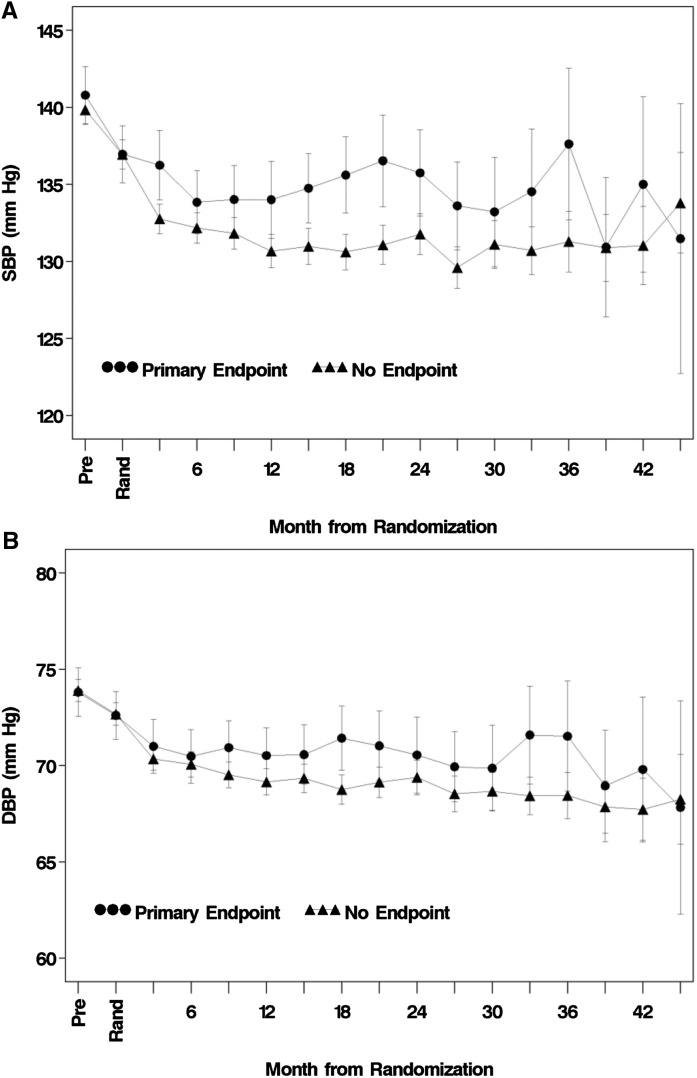
Design, setting, participants, & measurements: BP data from all 1448 randomized participants in the Veterans Affairs Nephropathy in Diabetes Trial were included in a post hoc analysis. The associations of mean on-treatment BP with the primary end point (decline in eGFR, ESRD, or death), renal end point (decline in eGFR or ESRD), rate of eGFR decline, and mortality were measured.
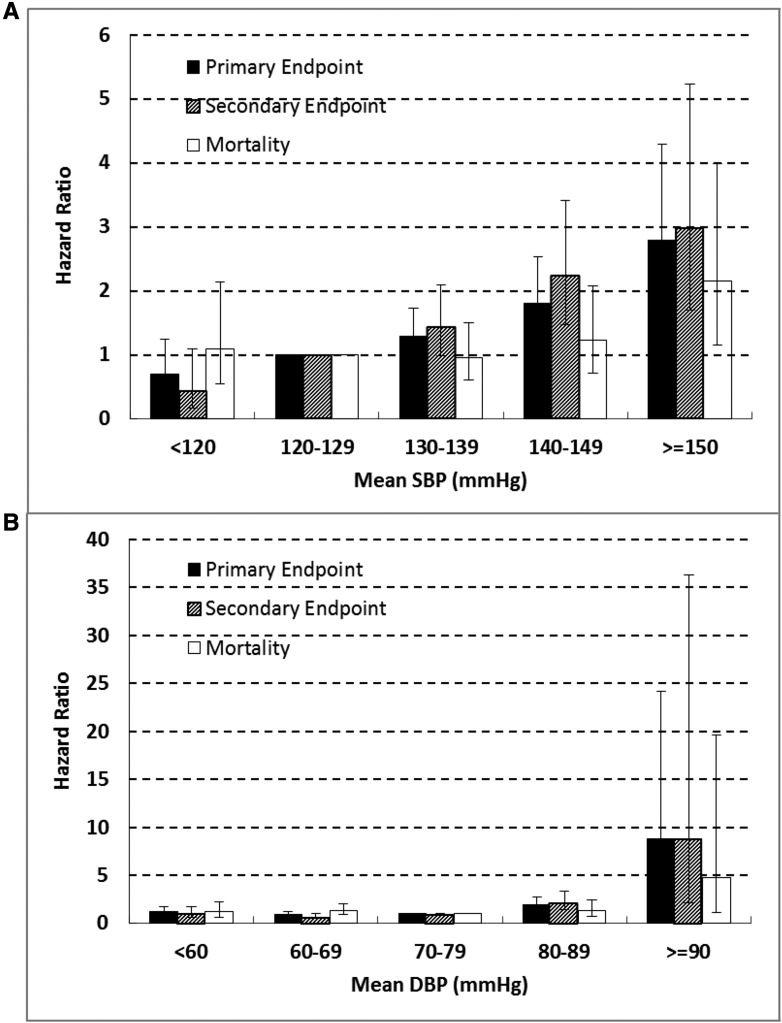
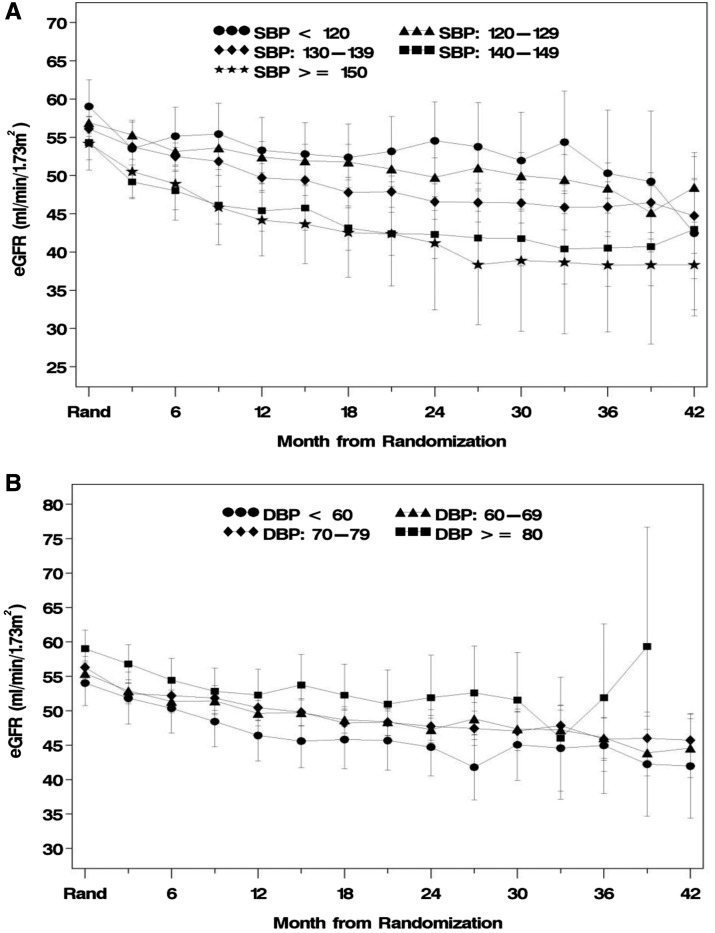
Results: The median (25th, 75th percentile) follow-up time was 2.2 (1.2, 3.0) years. There were 284 primary end points. In univariate analyses, both mean systolic and mean diastolic BPs were strongly associated (P<0.001) with the primary end point. After multivariate adjustment, the hazard of developing the primary end point became progressively higher as mean systolic BP rose from <120 to ≥ 150 mmHg (P=0.02), with a significantly higher hazard ratio for 140-149 versus 120-129 mmHg (1.51 [1.06, 2.15]; P=0.02). There was also a significant association of mean diastolic BP with the hazard of developing the primary end point (P<0.01), with a significantly higher hazard ratio when mean diastolic BP was 80-89 versus 70-79 mmHg (1.54 [1.05, 2.25]; P=0.03); there was also a strong trend when mean diastolic BP was <60 mmHg. Associations between BP and both renal end point and rate of eGFR decline were similar to those with the primary end point. No association of BP with mortality was observed, possibly because of the limited number of mortality events.
Conclusions: In patients with proteinuric diabetic kidney disease, mean systolic BP ≥ 140 mmHg and mean diastolic BP ≥ 80 mmHg were associated with worse renal outcomes.
Keywords: blood pressure; diabetes mellitus; diabetic nephropathies; end-stage renal disease; follow-up studies; glomerular filtration rate; humans; kidney failure, chronic; progression of chronic kidney disease; proteinuria.
Copyright © 2015 by the American Society of Nephrology.
Figures
Similar articles
-
Design of combination angiotensin receptor blocker and angiotensin-converting enzyme inhibitor for treatment of diabetic nephropathy (VA NEPHRON-D).Clin J Am Soc Nephrol. 2009 Feb;4(2):361-8. doi: 10.2215/CJN.03350708. Epub 2008 Dec 31. Clin J Am Soc Nephrol. 2009. PMID: 19118120 Free PMC article. Clinical Trial.
-
Effects of blood pressure level on progression of diabetic nephropathy: results from the RENAAL study.Arch Intern Med. 2003 Jul 14;163(13):1555-65. doi: 10.1001/archinte.163.13.1555. Arch Intern Med. 2003. PMID: 12860578 Clinical Trial.
-
Combined angiotensin inhibition for the treatment of diabetic nephropathy.N Engl J Med. 2013 Nov 14;369(20):1892-903. doi: 10.1056/NEJMoa1303154. Epub 2013 Nov 9. N Engl J Med. 2013. PMID: 24206457 Clinical Trial.
-
Losartan in diabetic nephropathy.Expert Rev Cardiovasc Ther. 2004 Jul;2(4):473-83. doi: 10.1586/14779072.2.4.473. Expert Rev Cardiovasc Ther. 2004. PMID: 15225108 Review.
-
Advances in the treatment of diabetic renal disease: focus on losartan.Curr Med Res Opin. 2004 Mar;20(3):333-40. doi: 10.1185/030079903125003107. Curr Med Res Opin. 2004. PMID: 15025842 Review.
Cited by
-
Diabetic kidney disease in type 2 diabetes: a review of pathogenic mechanisms, patient-related factors and therapeutic options.PeerJ. 2021 Apr 19;9:e11070. doi: 10.7717/peerj.11070. eCollection 2021. PeerJ. 2021. PMID: 33976959 Free PMC article.
-
11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes-2023.Diabetes Care. 2023 Jan 1;46(Suppl 1):S191-S202. doi: 10.2337/dc23-S011. Diabetes Care. 2023. PMID: 36507634 Free PMC article. Review.
-
Impact of Albumin-to-Creatinine Ratio Point-of-Care Testing on the Diagnosis and Management of Diabetic Kidney Disease.J Diabetes Sci Technol. 2023 Mar;17(2):428-438. doi: 10.1177/19322968211054520. Epub 2021 Oct 28. J Diabetes Sci Technol. 2023. PMID: 34709065 Free PMC article.
-
Effect of Long-Term Systolic Blood Pressure Trajectory on Kidney Damage in the Diabetic Population: A Prospective Study in a Community-Based Chinese Cohort.Chin Med J (Engl). 2018 May 20;131(10):1199-1205. doi: 10.4103/0366-6999.231528. Chin Med J (Engl). 2018. PMID: 29722339 Free PMC article.
-
Nomogram for the prediction of diabetic nephropathy risk among patients with type 2 diabetes mellitus based on a questionnaire and biochemical indicators: a retrospective study.Aging (Albany NY). 2020 Jun 2;12(11):10317-10336. doi: 10.18632/aging.103259. Epub 2020 Jun 2. Aging (Albany NY). 2020. PMID: 32484786 Free PMC article.
References
-
- US Renal Data System : USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2013
-
- Bakris GL: The importance of blood pressure control in the patient with diabetes. Am J Med 116[Suppl 5A]: 30S–38S, 2004 - PubMed
-
- Parving HH, Andersen AR, Smidt UM, Svendsen PA: Early aggressive antihypertensive treatment reduces rate of decline in kidney function in diabetic nephropathy. Lancet 1: 1175–1179, 1983 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
