

Survival in Patients With Severe Lymphopenia Following Treatment With Radiation and Chemotherapy for Newly Diagnosed Solid Tumors
- PMID: 26483062
- PMCID: PMC4778429
- DOI: 10.6004/jnccn.2015.0151
Survival in Patients With Severe Lymphopenia Following Treatment With Radiation and Chemotherapy for Newly Diagnosed Solid Tumors
Abstract
Background: The immune system plays an important role in cancer surveillance and therapy. Chemoradiation can cause severe treatment-related lymphopenia (TRL) (<500 cells/mm3) that is associated with reduced survival.
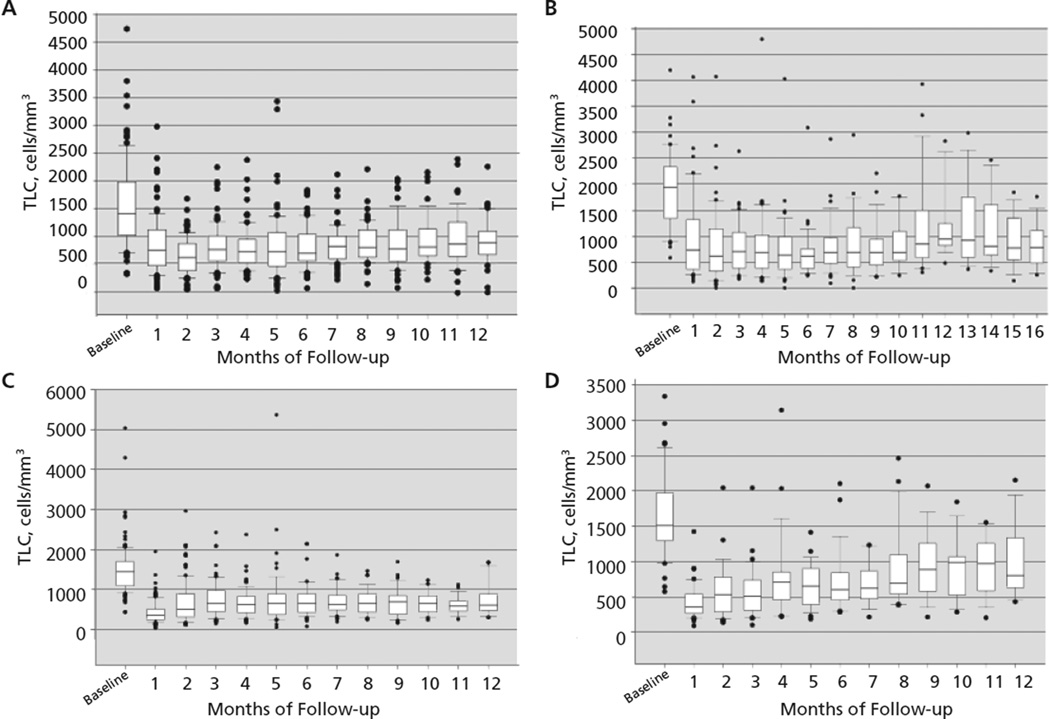
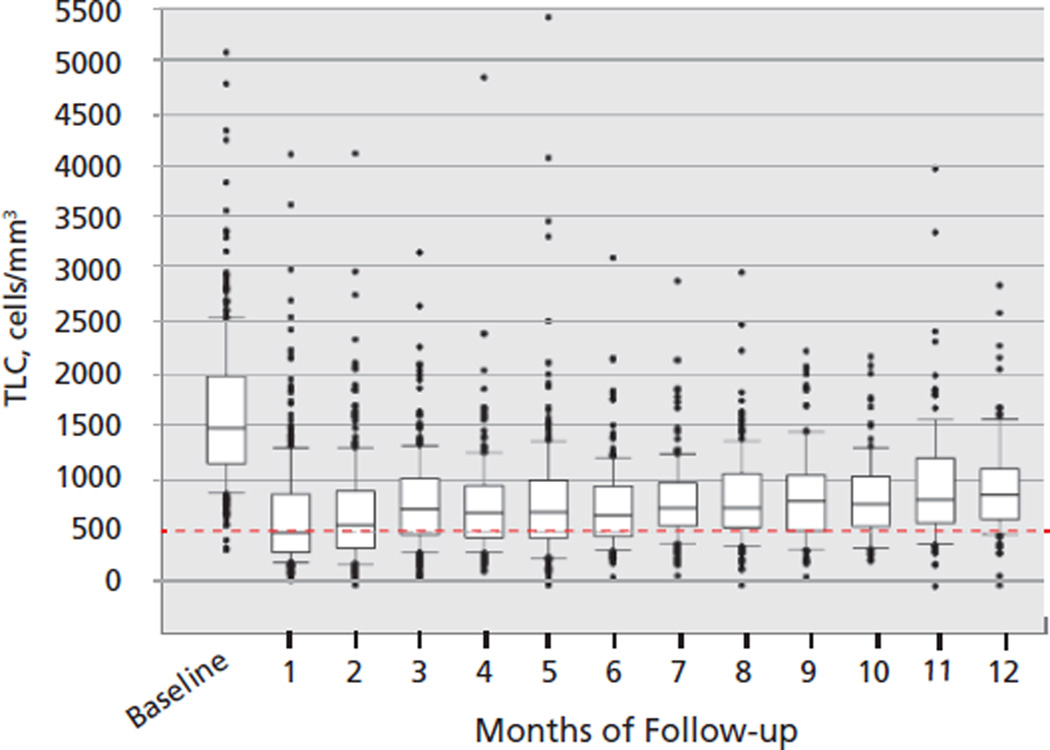
Materials and methods: Data from 4 independent solid tumor studies on serial lymphocyte counts, prognostic factors, treatment, and survival were collected and analyzed. The data set included 297 patients with newly diagnosed malignant glioma (N=96), resected pancreatic cancer (N=53), unresectable pancreatic cancer (N=101), and non-small cell lung cancer (N=47).
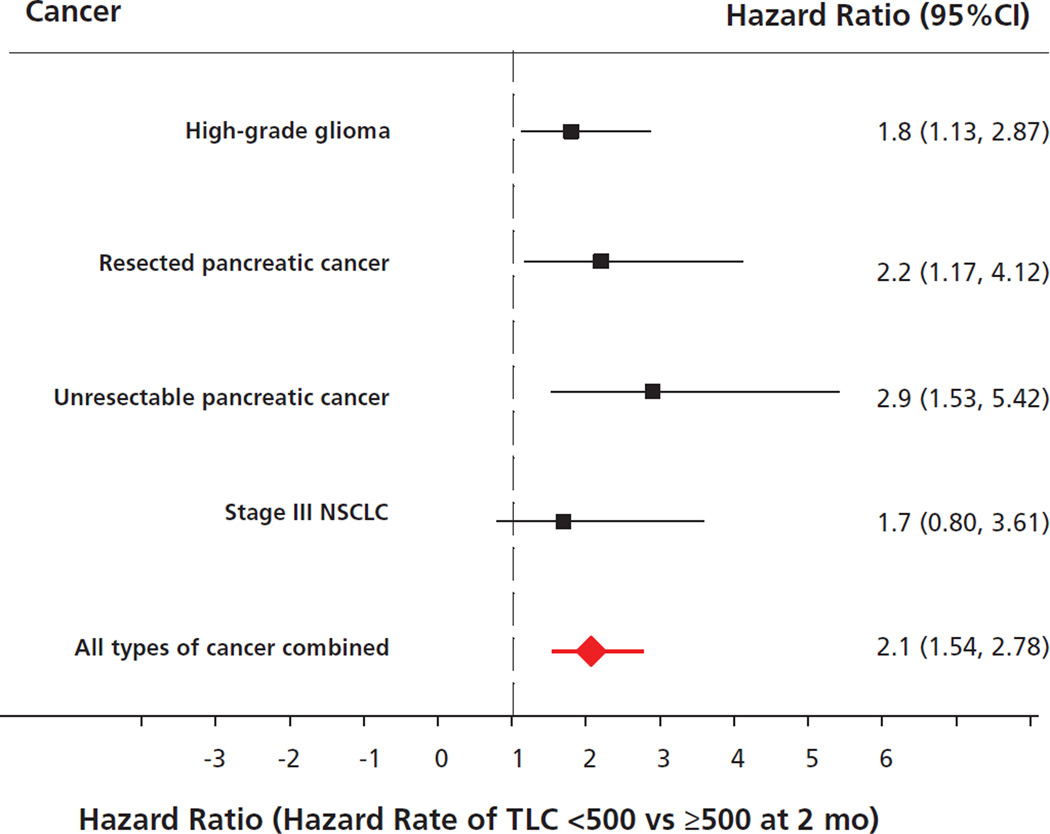
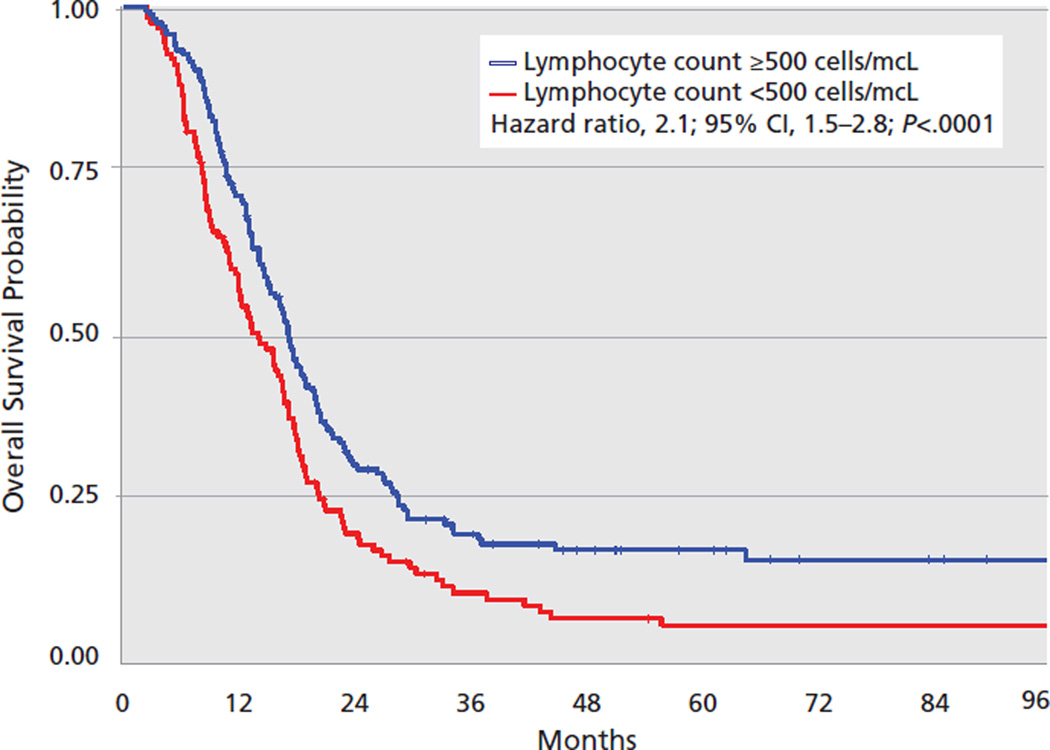
Results: Pretreatment lymphocyte counts were normal in 83% of the patient population, and no patient had severe baseline lymphopenia. Two months after initiating chemoradiation, 43% developed severe and persistent lymphopenia (P=.001). An increased risk for death was attributable to TRL in each cancer cohort (gliomas: hazard rate [HR], 1.8; 95% CI, 1.13-2.87; resected pancreas: HR, 2.2; 95% CI, 1.17-4.12; unresected pancreas: HR, 2.9; 95% CI, 1.53-5.42; and lung: HR, 1.7; 95% CI, 0.8-3.61) and in the entire study population regardless of pathologic findings (HR, 2.1; 95% CI, 1.54-2.78; P<.0001). Severe TRL was observed in more than 40% of patients 2 months after initiating chemoradiation, regardless of histology or chemotherapy regimen, and was independently associated with shorter survival from tumor progression.
Conclusions: Increased attention and research should be focused on the cause, prevention, and reversal of this unintended consequence of cancer treatment that seems to be related to survival in patients with solid tumors.
Copyright © 2015 by the National Comprehensive Cancer Network.
Figures
References
-
- Bremnes RM, Al-Shibli K, Donnem T, et al. The role of tumor-infiltrating immune cells and chronic inflammation at the tumor site on cancer development, progression, and prognosis: emphasis on non-small cell lung cancer. J Thorac Oncol. 2011;6:824–833. - PubMed
-
- Loi S, Sirtaine N, Piette F, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol. 2013;31:860–867. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
