

Atypical Bilateral Fuchs Uveitis: Diagnostic Challenges
- PMID: 26483668
- PMCID: PMC4608646
- DOI: 10.1159/000439081
Atypical Bilateral Fuchs Uveitis: Diagnostic Challenges
Abstract
Bilateral Fuchs uveitis associated with vitreous infiltration and posterior segment involvement requires a thorough diagnostic evaluation. The lack of well-defined diagnostic criteria makes identification of this entity difficult. The aim of this case report was to present the characteristics of a patient with atypical Fuchs uveitis and the procedures needed to rule out the differential diagnosis with specific attention to the utility of in vivo confocal microscopy (IVCM).
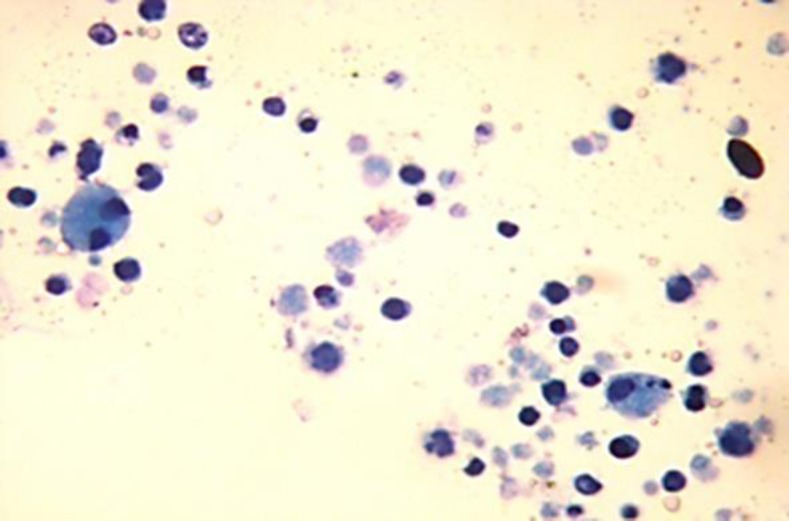
Case report: One case of chronic bilateral uveitis with severe vitreous opacities is presented. After extensive systemic workup, including vitrectomy, the case had no identifiable systemic etiology. IVCM of the cornea revealed the presence of dendritiform keratic precipitates.
Conclusion: The diagnosis of Fuchs uveitis is based on clinical findings as no confirmatory laboratory tests are available. A high index of suspicion is key to an early diagnosis, especially in the cases with vitreous opacities and posterior segment manifestations. Auxiliary tests such as IVCM may aid the clinician in the diagnosis of Fuchs uveitis.
Keywords: Bilateral Fuchs uveitis; Diagnosis; In vivo confocal microscopy.
Figures


References
-
- Kazokoglu H, Onal S, Tugal-Tutkun I, et al. Demographic and clinical features of uveitis in tertiary centers in Turkey. Ophthalmic Epidemiol. 2008;15:285–293. - PubMed
-
- Mohamed Q, Zamir E. Update on Fuchs' uveitis syndrome. Curr Opin Ophthalmol. 2005;16:356–363. - PubMed
-
- La Hey E, Baarsma GS, de Vries J, Kijlstra A. Clinical analysis of Fuchs heterochromic cyclitis. Doc Ophthalmol. 1991;78:225–235. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
