

Sporadic nocturnal frontal lobe epilepsy: A consecutive series of 8 cases
- PMID: 26483923
- PMCID: PMC4559607
- DOI: 10.1016/j.slsci.2014.09.016
Sporadic nocturnal frontal lobe epilepsy: A consecutive series of 8 cases
Abstract
Objective: To present findings on a series of cases of sporadic nocturnal frontal lobe epilepsy (NFLE), a form of NFLE that is infrequently reported, in contrast to familial (autosomal dominant) NFLE. Both forms of NFLE need to be distinguished from parasomnias, nocturnal temporal lobe epilepsy, and other nocturnal disorders.
Methods: Eight consecutive cases of sporadic NFLE were evaluated at a sleep clinic in Taiwan. All patients had clinical evaluations, daytime waking and sleeping EEGs, brain MRIs, and overnight video-polysomnography (vPSG) with seizure montage.
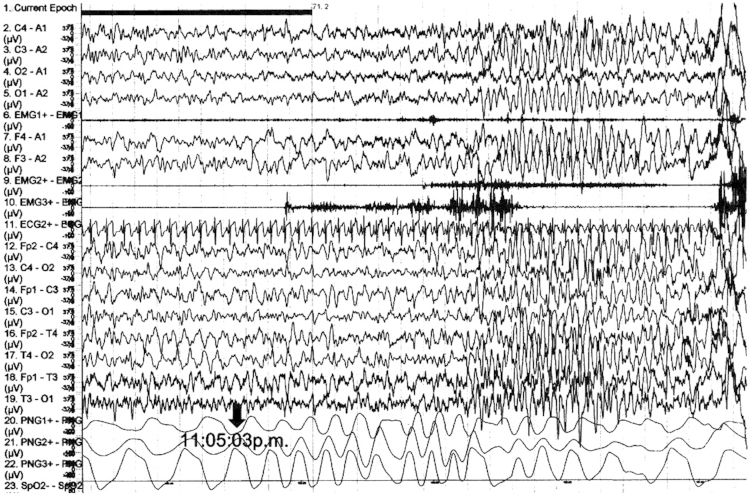
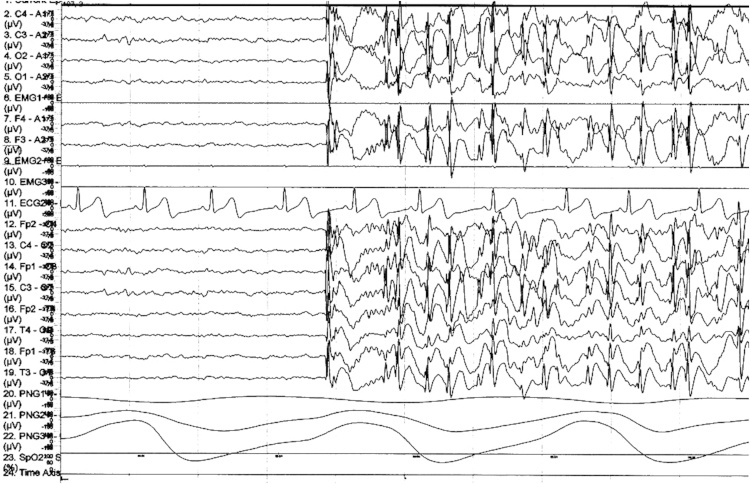
Results: Gender was equal (four males, four females); mean age was 18.4 yrs (range, 7-41 yrs). Age of NFLE onset was by puberty. Premorbid history was negative for any neurologic, medical or psychiatric disorder. NFLE subtypes: nocturnal paroxysmal dystonia, n=6; paroxysmal arousals, n=2. MRI brain scan abnormalities with clinical correlates were found in one patient. Daytime awake EEGs were negative for ictal/interictal activity in all patients, but two patients had daytime sleep EEGs with interictal epileptiform EEG activity. During vPSG studies, three of eight patients with NFLE seizure events had concurrent epileptiform EEG activity, and two patients had interictal epileptiform EEG activity during their vPSG studies. No case had a spontaneous remission. Anticonvulsant therapy was highly effective in all eight cases (>75% reduction in seizure frequency).
Discussion: These cases confirm that sporadic NFLE closely resembles familial NFLE, and comprises a set of distinct clinical manifestations, with variable intensity, and variable scalp EEG epileptiform abnormalities across sleep and wakefulness, which have previously been identified in Caucasian patients from Europe and North America.
Keywords: Anticonvulsant therapy; Nocturnal frontal lobe epilepsy (sporadic, familial); Nocturnal paroxysmal dystonia; Nocturnal temporal lobe epilepsy; Paroxysmal arousals; Video-polysomnography.
Figures
Similar articles
-
Sporadic Nocturnal Frontal Lobe Epilepsy--Report on Two Cases and Review of the First Taiwanese Series of 10 Cases.Acta Neurol Taiwan. 2017 Jun 15;26(2):55-63. Acta Neurol Taiwan. 2017. PMID: 29250756 Review.
-
Nocturnal frontal lobe epilepsy. A clinical and polygraphic overview of 100 consecutive cases.Brain. 1999 Jun;122 ( Pt 6):1017-31. doi: 10.1093/brain/122.6.1017. Brain. 1999. PMID: 10356056
-
The wide clinical spectrum of nocturnal frontal lobe epilepsy.Sleep Med Rev. 2000 Aug;4(4):375-386. doi: 10.1053/smrv.2000.0109. Sleep Med Rev. 2000. PMID: 12531176
-
Complex nocturnal behaviors: nocturnal seizures and parasomnias.Continuum (Minneap Minn). 2013 Feb;19(1 Sleep Disorders):104-31. doi: 10.1212/01.CON.0000427210.98305.8f. Continuum (Minneap Minn). 2013. PMID: 23385697 Review.
-
Diagnosing nocturnal frontal lobe epilepsy: a case study of two children.Seizure. 2011 Sep;20(7):583-5. doi: 10.1016/j.seizure.2011.03.004. Epub 2011 Apr 21. Seizure. 2011. PMID: 21511499
Cited by
-
Sleep-related hypermotor epilepsy-No longer controversial.Epilepsia. 2025 Jul;66(7):2182-2189. doi: 10.1111/epi.18364. Epub 2025 Mar 14. Epilepsia. 2025. PMID: 40085429 Free PMC article. No abstract available.
-
Alcohol dependent and GTCS patient with sleep-related hyper motor epilepsy.Ind Psychiatry J. 2025 Jan-Apr;34(1):133-135. doi: 10.4103/ipj.ipj_183_24. Epub 2025 Jan 15. Ind Psychiatry J. 2025. PMID: 40376635 Free PMC article. No abstract available.
-
The far side of sleep: Towards a deeper understanding of parasomnias and nocturnal seizures.Sleep Sci. 2014 Sep;7(3):129-34. doi: 10.1016/j.slsci.2014.11.006. Epub 2014 Dec 15. Sleep Sci. 2014. PMID: 26483917 Free PMC article. No abstract available.
-
Sleep Related Epilepsy and Pharmacotherapy: An Insight.Front Pharmacol. 2018 Sep 27;9:1088. doi: 10.3389/fphar.2018.01088. eCollection 2018. Front Pharmacol. 2018. PMID: 30319421 Free PMC article. Review.
References
-
- Passouant P. Historical aspects of sleep and epilepsy. Epilepsy Res. 1991;2:19–22. - PubMed
-
- Young GB, Blume WT, Wells GA. Differential aspects of sleep epilepsy. Can J Neurol Sci. 1985;12:317–320. - PubMed
-
- Derry CP, Duncan JS, Berkovic SF. Paroxysmal motor disorders of sleep: the clinical spectrum and differentiation from epilepsy. Epilepsia. 2006;47:1775–1791. - PubMed
-
- Bernasconi A, Andermann F, Cendes F. Nocturnal temporal lobe epilepsy. Neurology. 1998;50:1772–1777. - PubMed
-
- Provini F, Plazzi G, Tinuper P. Nocturnal frontal lobe epilepsy: A clinical and polygraphic overview of 100 consecutive cases. Brain. 1999;122:1017–1031. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
