

Evans Syndrome in Children: Long-Term Outcome in a Prospective French National Observational Cohort
- PMID: 26484337
- PMCID: PMC4586429
- DOI: 10.3389/fped.2015.00079
Evans Syndrome in Children: Long-Term Outcome in a Prospective French National Observational Cohort
Abstract
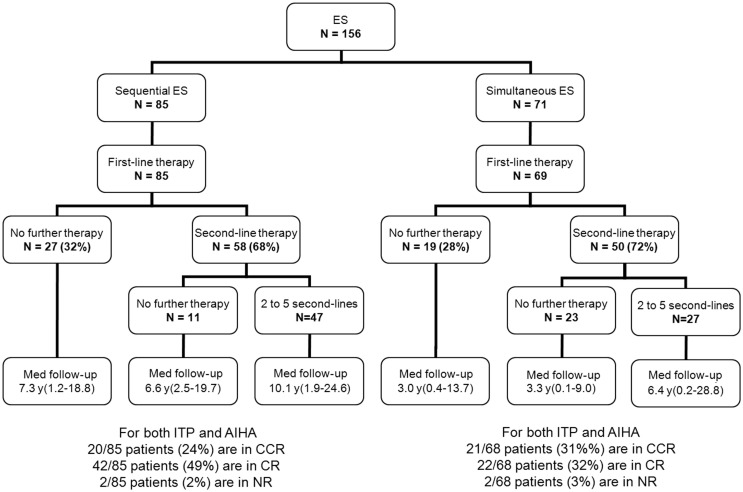
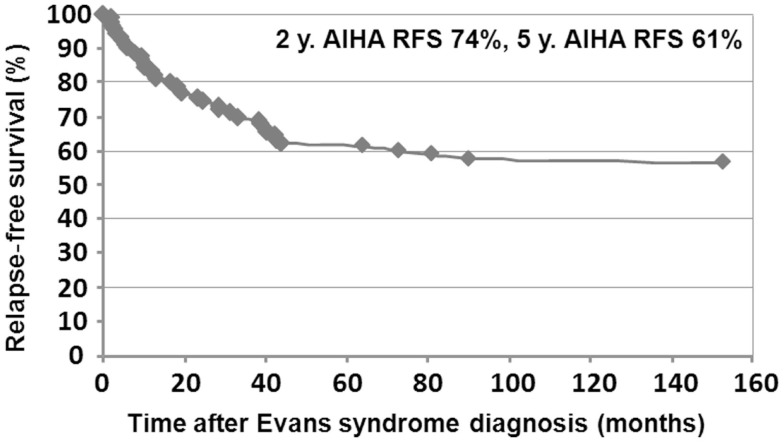
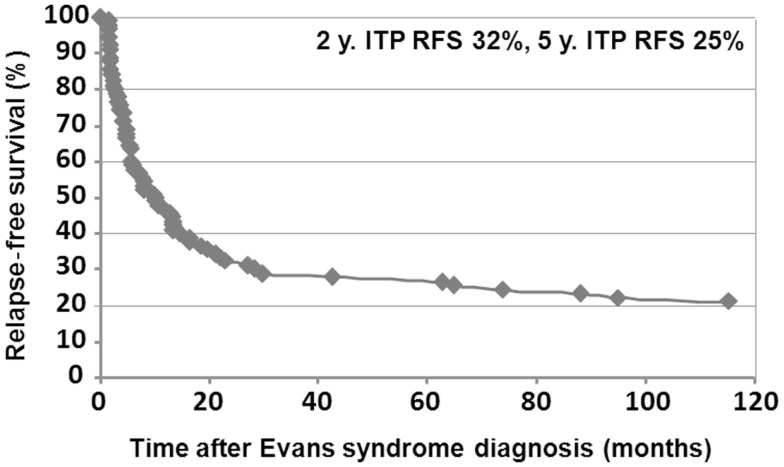
Evans syndrome (ES) is a rare autoimmune disorder whose long-term outcome is not well known. In France, a collaborative pediatric network set up via the National Rare Disease Plan now provides comprehensive clinical data in children with this disease. Patients aged less than 18 years at the initial presentation of autoimmune cytopenia have been prospectively included into a national observational cohort since 2004. The definition of ES was restricted to the simultaneous or sequential association of autoimmune hemolytic anemia (AIHA) and immune thrombocytopenic purpura (ITP). Cases were deemed secondary if associated with a primitive immunodeficiency or systemic lupus erythematosus. In December 2014, we analyzed the data pertaining to 156 children from 26 centers with ES whose diagnosis was made between 1981 and 2014. Median age (range) at the onset of cytopenia was 5.4 years (0.2-17.2). In 85 sequential cases, the time lapse between the first episodes of AIHA and ITP was 2.4 years (0.1-16.3). The follow-up period as from ES diagnosis was 6.5 years (0.1-28.8). ES was secondary, revealing another underlying disease, in 10% of cases; various associated immune manifestations (mainly lymphoproliferation, other autoimmune diseases, and hypogammaglobulinemia) were observed in 60% of cases; and ES remained primary in 30% of cases. Five-year ITP and AIHA relapse-free survival were 25 and 61%, respectively. Overall, 69% of children required one or more second-line immune treatments, and 15 patients (10%) died at the age of 14.3 years (1.7-28.1). To our knowledge, this is the first consistent long-term clinical description of this rare syndrome. It underscores the high rate of associated immune manifestations and the burden of long-term complications and treatment toxicity. Future challenges include (1) the identification of the underlying genetic defects inducing immune dysregulation and (2) the need to better characterize patient subgroups and second-line treatment strategies.
Keywords: Evans syndrome; autoimmune hemolytic anemia; child; immune thrombocytopenic purpura.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources