

Reductions in Sepsis Mortality and Costs After Design and Implementation of a Nurse-Based Early Recognition and Response Program
- PMID: 26484679
- PMCID: PMC4880050
- DOI: 10.1016/s1553-7250(15)41063-3
Reductions in Sepsis Mortality and Costs After Design and Implementation of a Nurse-Based Early Recognition and Response Program
Abstract
Background: Sepsis is a leading cause of death, but evidence suggests that early recognition and prompt intervention can save lives. In 2005 Houston Methodist Hospital prioritized sepsis detection and management in its ICU. In late 2007, because of marginal effects on sepsis death rates, the focus shifted to designing a program that would be readily used by nurses and ensure early recognition of patients showing signs suspicious for sepsis, as well as the institution of prompt, evidence-based interventions to diagnose and treat it.
Methods: The intervention had four components: organizational commitment and data-based leadership; development and integration of an early sepsis screening tool into the electronic health record; creation of screening and response protocols; and education and training of nurses. Twice-daily screening of patients on targeted units was conducted by bedside nurses; nurse practitioners initiated definitive treatment as indicated. Evaluation focused on extent of implementation, trends in inpatient mortality, and, for Medicare beneficiaries, a before-after (2008-2011) comparison of outcomes and costs. A federal grant in 2012 enabled expansion of the program.
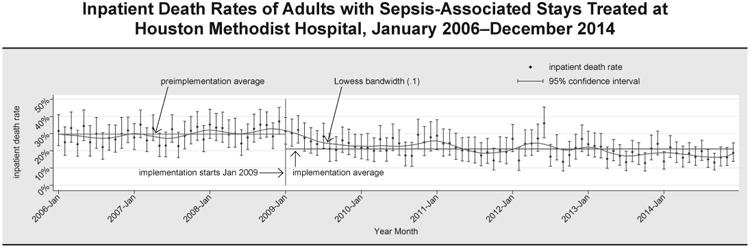
Results: By year 3 (2011) 33% of inpatients were screened (56,190 screens in 9,718 unique patients), up from 10% in year 1 (2009). Inpatient sepsis-associated death rates decreased from 29.7% in the preimplementation period (2006-2008) to 21.1% after implementation (2009-2014). Death rates and hospital costs for Medicare beneficiaries decreased from preimplementation levels without a compensatory increase in discharges to postacute care.
Conclusion: This program has been associated with lower inpatient death rates and costs. Further testing of the robustness and exportability of the program is under way.
Figures
Similar articles
-
Using the integrated nurse leadership program to reduce sepsis mortality.Jt Comm J Qual Patient Saf. 2015 Jun;41(6):264-72. doi: 10.1016/s1553-7250(15)41036-0. Jt Comm J Qual Patient Saf. 2015. PMID: 25990892
-
Clinical imperative versus economic consequence: exploring the cost burden and opportunities in the care of patients with sepsis.Nurs Adm Q. 2011 Jan-Mar;35(1):61-7. doi: 10.1097/NAQ.0b013e318203498d. Nurs Adm Q. 2011. PMID: 21157265
-
Implementation of a Value-Driven Outcomes Program to Identify High Variability in Clinical Costs and Outcomes and Association With Reduced Cost and Improved Quality.JAMA. 2016 Sep 13;316(10):1061-72. doi: 10.1001/jama.2016.12226. JAMA. 2016. PMID: 27623461
-
Evidenced-based practice: priorities and implementation strategies.AACN Clin Issues. 2005 Jan-Mar;16(1):36-42. doi: 10.1097/00044067-200501000-00005. AACN Clin Issues. 2005. PMID: 15714016 Review.
-
Preventing Harm in the ICU-Building a Culture of Safety and Engaging Patients and Families.Crit Care Med. 2017 Sep;45(9):1531-1537. doi: 10.1097/CCM.0000000000002556. Crit Care Med. 2017. PMID: 28640023 Review.
Cited by
-
Near-simultaneous intensive care unit (ICU) admissions and all-cause mortality: a cohort study.Intensive Care Med. 2019 Nov;45(11):1559-1569. doi: 10.1007/s00134-019-05753-4. Epub 2019 Sep 17. Intensive Care Med. 2019. PMID: 31531716
-
Information displays for automated surveillance algorithms of in-hospital patient deterioration: a scoping review.J Am Med Inform Assoc. 2023 Dec 22;31(1):256-273. doi: 10.1093/jamia/ocad203. J Am Med Inform Assoc. 2023. PMID: 37847664 Free PMC article.
-
Considerations for Empiric Antimicrobial Therapy in Sepsis and Septic Shock in an Era of Antimicrobial Resistance.J Infect Dis. 2020 Jul 21;222(Suppl 2):S119-S131. doi: 10.1093/infdis/jiaa221. J Infect Dis. 2020. PMID: 32691833 Free PMC article.
-
Promoting early identification of sepsis in hospitalized patients with nurse-led protocols.Crit Care. 2017 Jan 11;21(1):10. doi: 10.1186/s13054-016-1590-0. Crit Care. 2017. PMID: 28073375 Free PMC article. No abstract available.
-
Sepsis in Burns-Lessons Learnt from Developments in the Management of Septic Shock.Medicina (Kaunas). 2021 Dec 24;58(1):26. doi: 10.3390/medicina58010026. Medicina (Kaunas). 2021. PMID: 35056334 Free PMC article. Review.
References
-
- Centers for Disease Control and Prevention. National Vital Statistics System: Leading Causes of Death. [Accessed Oct 1, 2015]; http://www.cdc.gov/nchs/data/dvs/LCWK9_2013.pdf. - PubMed
-
- Centers for Disease Control and Prevention, National Vital Statistics System, National Center for Health Statistics. Ten Leading Causes of Death and Injury by Age Group, United States—2013. [Accessed Oct 1, 2015]; http://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_by_ag.... - PubMed
-
- Agency for Healthcare Research and Quality. HCUP Statistical Brief 160. Torio CM, Andrews RM. [Accessed Sep 24, 2015];National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011. 2013 Aug; http://www.hcup-us.ahrq.gov/reports/statbriefs/sb160.pdf. - PubMed
-
- Rangel-Frausto MS, et al. The natural history of the systemic Inflammatory response syndrome (SIRS). A prospective study. JAMA. 1995 Jan 11;273(2):117–123. - PubMed
-
- Dellinger RP, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
