

Meconium aspiration syndrome: a role for fetal systemic inflammation
- PMID: 26484777
- PMCID: PMC5625352
- DOI: 10.1016/j.ajog.2015.10.009
Meconium aspiration syndrome: a role for fetal systemic inflammation
Abstract
Background: Meconium aspiration syndrome (MAS) is a leading cause of morbidity and mortality in term infants. Meconium-stained amniotic fluid (MSAF) occurs in approximately 1 of every 7 pregnancies, but only 5% of neonates exposed to MSAF develop MAS. Why some infants exposed to meconium develop MAS while others do not is a fundamental question. Patients with MSAF have a higher frequency of intraamniotic inflammation/infection than those with clear fluid. We propose that fetal systemic inflammation is a risk factor for the development of MAS in patients with MSAF.
Objective: We sought to investigate whether intraamniotic inflammation and funisitis, the histopathologic landmark of a fetal inflammatory response, predispose to MAS.
Study design: A prospective cohort study was conducted from 1995 through 2009. Amniotic fluid (AF) samples (n = 1281) were collected at the time of cesarean delivery from women who delivered singleton newborns at term (gestational age ≥38 weeks). Intraamniotic inflammation was diagnosed if the AF concentration of matrix metalloproteinase-8 was >23 ng/mL. Funisitis was diagnosed by histologic examination if inflammation was present in the umbilical cord.
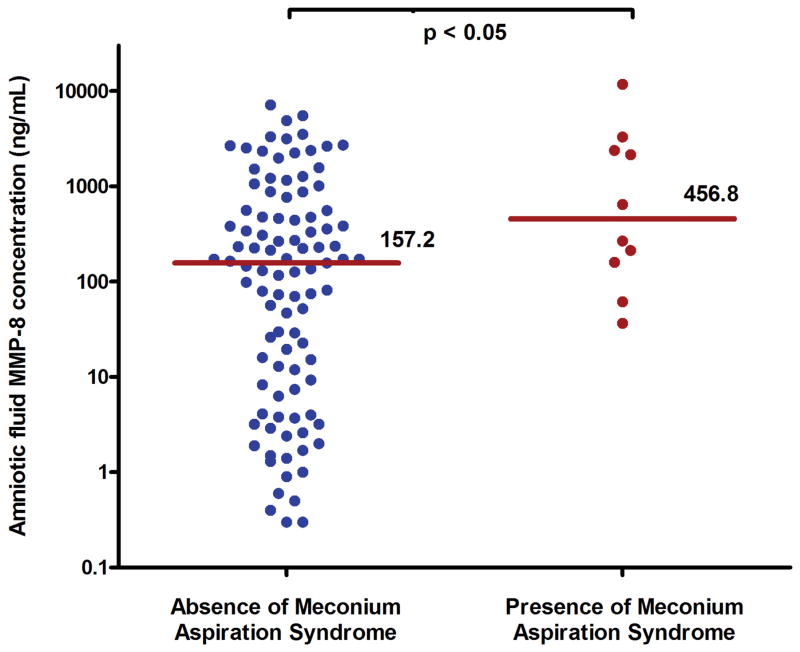
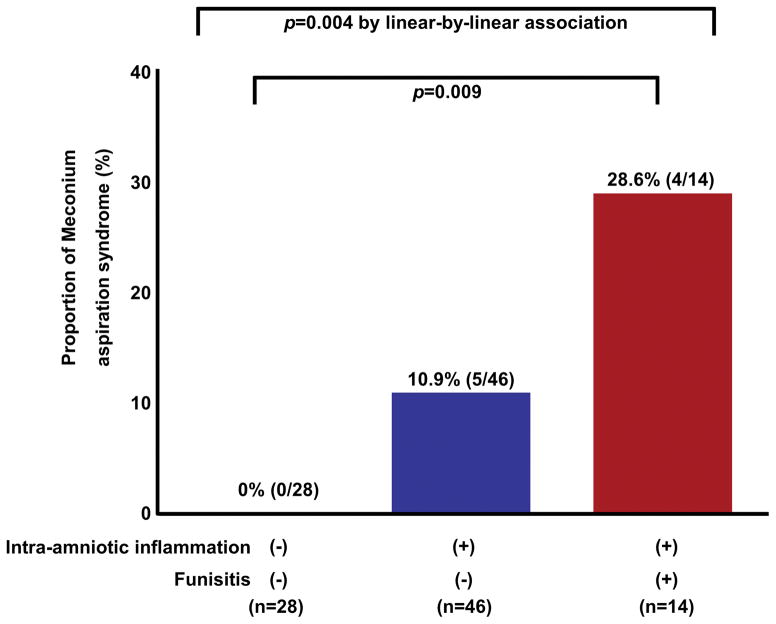
Results: The prevalence of MSAF was 9.2% (118/1281), and 10.2% (12/118) of neonates exposed to MSAF developed MAS. There were no significant differences in the median gestational age or umbilical cord arterial pH at birth between neonates who developed MAS and those who did not (each P > .1). Mothers whose newborns developed MAS had a higher median of AF matrix metalloproteinase-8 (456.8 vs 157.2 ng/mL, P < .05). Newborns exposed to intraamniotic inflammation had a higher rate of MAS than those who were not exposed to intraamniotic inflammation [13.0% (10/77) vs 0% (0/32), P = .03], as did those exposed to funisitis [31.3% (5/16) vs 7.3% (6/82); relative risk, 4.3; 95% confidence interval, 1.5-12.3]. Among the 89 newborns for whom both AF and placental histology were available, MAS was more common in patients with both intraamniotic inflammation and funisitis than in those without intraamniotic inflammation and funisitis [28.6% (4/14) vs 0% (0/28), P = .009], while the rate of MAS did not show a significant difference between patients with intraamniotic inflammation alone (without funisitis) and those without intraamniotic inflammation and funisitis [10.9% (5/46) vs 0% (0/28)].
Conclusion: The combination of intraamniotic inflammation with fetal systemic inflammation is an important antecedent of MAS. This concept has implications for the understanding of the mechanisms of disease responsible for MAS and for the development of prognostic models and therapeutic interventions for this disorder.
Keywords: amniocentesis; fetal inflammatory response syndrome; funisitis; intraamniotic inflammation; matrix metalloproteinase-8; meconium-stained amniotic fluid; pregnancy.
Published by Elsevier Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Meconium aspiration syndrome: do we know?Turk J Pediatr. 2011 Mar-Apr;53(2):121-9. Turk J Pediatr. 2011. PMID: 21853647 Review.
-
Secreted phospholipase A2 is increased in meconium-stained amniotic fluid of term gestations: potential implications for the genesis of meconium aspiration syndrome.J Matern Fetal Neonatal Med. 2014 Jul;27(10):975-83. doi: 10.3109/14767058.2013.847918. Epub 2014 Jan 6. J Matern Fetal Neonatal Med. 2014. PMID: 24063538 Free PMC article.
-
Influence of foetal inflammation on the development of meconium aspiration syndrome in term neonates with meconium-stained amniotic fluid.PeerJ. 2019 May 31;7:e7049. doi: 10.7717/peerj.7049. eCollection 2019. PeerJ. 2019. PMID: 31183262 Free PMC article.
-
Meconium-stained amniotic fluid and neonatal morbidity in near-term and term deliveries with acute histologic chorioamnionitis and/or funisitis.J Perinatol. 2001 Dec;21(8):537-40. doi: 10.1038/sj.jp.7210564. J Perinatol. 2001. PMID: 11774015
-
Clinical chorioamnionitis at term: definition, pathogenesis, microbiology, diagnosis, and treatment.Am J Obstet Gynecol. 2024 Mar;230(3S):S807-S840. doi: 10.1016/j.ajog.2023.02.002. Epub 2023 Mar 21. Am J Obstet Gynecol. 2024. PMID: 38233317 Free PMC article. Review.
Cited by
-
Evidence of both foetal inflammation and hypoxia-ischaemia is associated with meconium aspiration syndrome.Sci Rep. 2021 Aug 18;11(1):16799. doi: 10.1038/s41598-021-96275-x. Sci Rep. 2021. PMID: 34408219 Free PMC article.
-
Are amniotic fluid neutrophils in women with intraamniotic infection and/or inflammation of fetal or maternal origin?Am J Obstet Gynecol. 2017 Dec;217(6):693.e1-693.e16. doi: 10.1016/j.ajog.2017.09.013. Epub 2017 Sep 28. Am J Obstet Gynecol. 2017. PMID: 28964823 Free PMC article.
-
Does the human placenta delivered at term have a microbiota? Results of cultivation, quantitative real-time PCR, 16S rRNA gene sequencing, and metagenomics.Am J Obstet Gynecol. 2019 Mar;220(3):267.e1-267.e39. doi: 10.1016/j.ajog.2018.10.018. Am J Obstet Gynecol. 2019. PMID: 30832984 Free PMC article.
-
Placental Lesions in Meconium Aspiration Syndrome.J Pathol Transl Med. 2017 Sep;51(5):488-498. doi: 10.4132/jptm.2017.07.20. Epub 2017 Aug 9. J Pathol Transl Med. 2017. PMID: 28793392 Free PMC article.
-
HSP70: an alarmin that does not induce high rates of preterm birth but does cause adverse neonatal outcomes.J Matern Fetal Neonatal Med. 2021 Dec;34(24):4110-4118. doi: 10.1080/14767058.2019.1706470. Epub 2020 Jan 6. J Matern Fetal Neonatal Med. 2021. PMID: 31906756 Free PMC article.
References
-
- Dargaville PA, Copnell B. The epidemiology of meconium aspiration syndrome: incidence, risk factors, therapies, and outcome. Pediatrics. 2006;117:1712–21. - PubMed
-
- Wiswell TE. Delivery room management of the meconium-stained newborn. J Perinatol. 2008;28(Suppl 3):S19–26. - PubMed
-
- Srinivasan HB, Vidyasagar D. Meconium aspiration syndrome: current concepts and management. Compr Ther. 1999;25:82–9. - PubMed
-
- Vidyasagar D, Lukkarinen H, Kaapa P, Zagariya A. Inflammatory response and apoptosis in newborn lungs after meconium aspiration. Biotechnol Prog. 2005;21:192–7. - PubMed
-
- Bhat R, Vidyasagar D. Delivery room management of meconium-stained infant. Clin Perinatol. 2012;39:817–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
