

Variation in attrition at subnational level: review of the Botswana National HIV/AIDS Treatment (Masa) programme data (2002-2013)
- PMID: 26485172
- PMCID: PMC4834839
- DOI: 10.1111/tmi.12623
Variation in attrition at subnational level: review of the Botswana National HIV/AIDS Treatment (Masa) programme data (2002-2013)
Abstract
Objective: To evaluate the variation in all-cause attrition [mortality and loss to follow-up (LTFU)] among HIV-infected individuals in Botswana by health district during the rapid and massive scale-up of the National Treatment Program.
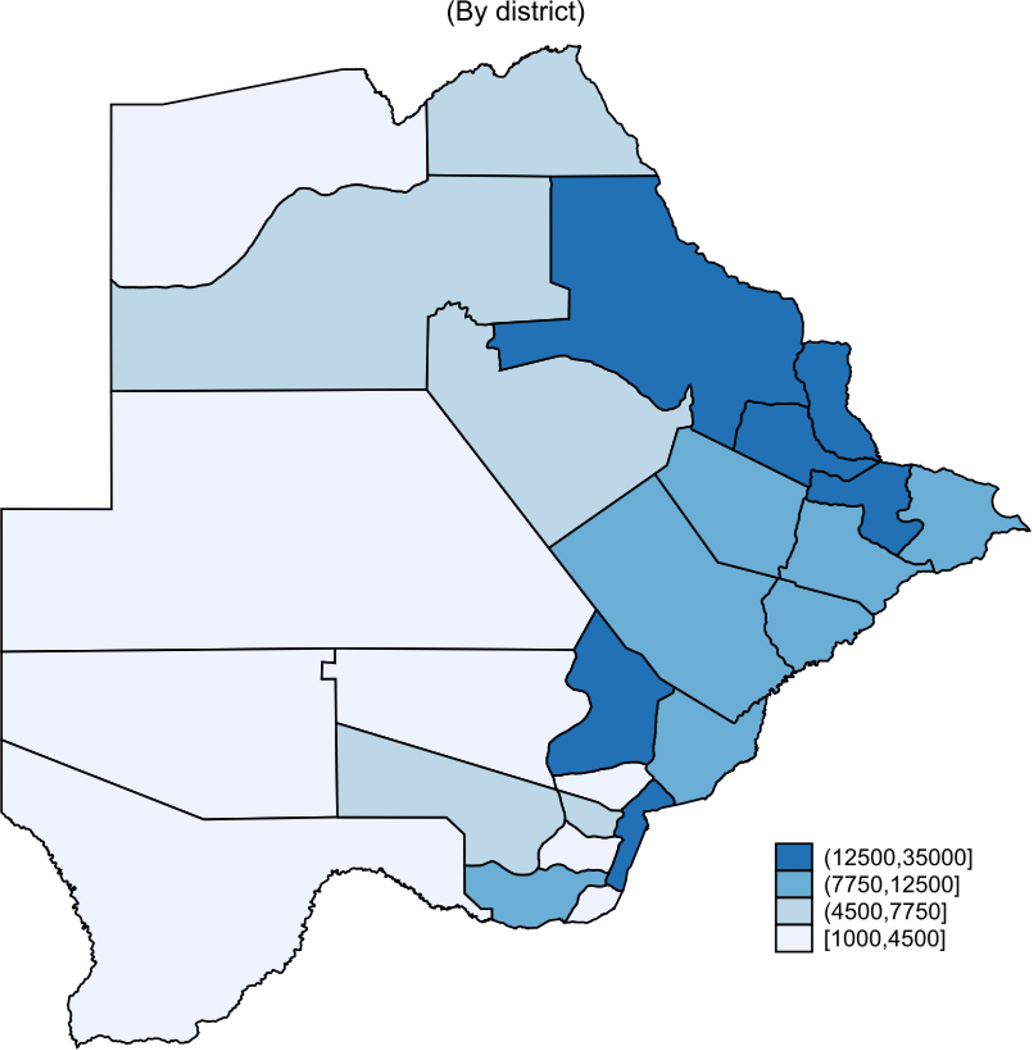
Methods: Analysis of routinely collected longitudinal data from 226 030 patients who received ART through the Botswana National HIV/AIDS Treatment Program across all 24 health districts from 2002 to 2013. A time-to-event analysis was used to measure crude mortality and loss to follow-up rates (LTFU). A marginal structural model was used to evaluate mortality and LTFU rates by district over time, adjusted for individual-level risk factors (e.g. age, gender, baseline CD4, year of treatment initiation and antiretroviral regimen).
Results: Mortality rates in the districts ranged from the lowest 1.0 (95% CI 0.9-1.1) in Selibe-Phikwe, to the highest 5.0 (95% CI 4.0-6.1), in Mabutsane. There was a wide range of overall LTFU across districts, including rates as low as 4.6 (95% CI 4.4-4.9) losses per 100 person-years in Ngamiland, and 5.9 (95% CI 5.6-6.2) losses per 100 person-years in South East district, to rates as high as 25.4 (95% CI 23.08-27.89) losses per 100 person-years in Mabutsane and 46.3 (95% CI 43.48-49.23) losses per 100 person-years in Okavango. Even when known risk factors for mortality and LTFU were adjusted for, district was a significant predictor of both mortality and LTFU rates.
Conclusion: We found statistically significant variation in attrition (mortality and LTFU) and data quality among districts. These findings suggest that district-level contextual factors affect retention in treatment. Further research needs to investigate factors that can potentially cause this variation.
Keywords: ART; HIV; TAR; VIH; Botswana; abandono; antiretroviral therapy; attrition; marginal structural model; modelo estructural marginal; modèle structurel marginal; multilevel; multinivel; à plusieurs niveaux.
© 2015 John Wiley & Sons Ltd.
Figures
References
-
- Atun R, Bataringaya J. Building a durable response to HIV/AIDS: implications for health systems. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2011;57:S91–S95. - PubMed
-
- WHO. Global update on HIV treatment 2013: results, impact and opportunities. Geneva: World Health Organization; 2013.
-
- M & E Unit. Monitoring & Evaluation Unit Monthly Report Feb. 2015. Gaborone, Botswana: Ministry of Health; 2015.
-
- Farahani M, Vable A, Lebelonyane R, Seipone K, Anderson M, Avalos A, et al. Outcomes of the Botswana national HIV/AIDS treatment programme from 2002 to 2010: a longitudinal analysis. The lancet global health. 2014;2:e44–e50. - PubMed
-
- Govindasamy D, Kranzer K, Ford N. Strengthening the HIV cascade to ensure an effective future ART response in sub-Saharan Africa. Transactions of The Royal Society of Tropical Medicine and Hygiene. 2014;108:1–3. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
