

MiR-486 and miR-92a Identified in Circulating HDL Discriminate between Stable and Vulnerable Coronary Artery Disease Patients
- PMID: 26485305
- PMCID: PMC4617647
- DOI: 10.1371/journal.pone.0140958
MiR-486 and miR-92a Identified in Circulating HDL Discriminate between Stable and Vulnerable Coronary Artery Disease Patients
Abstract
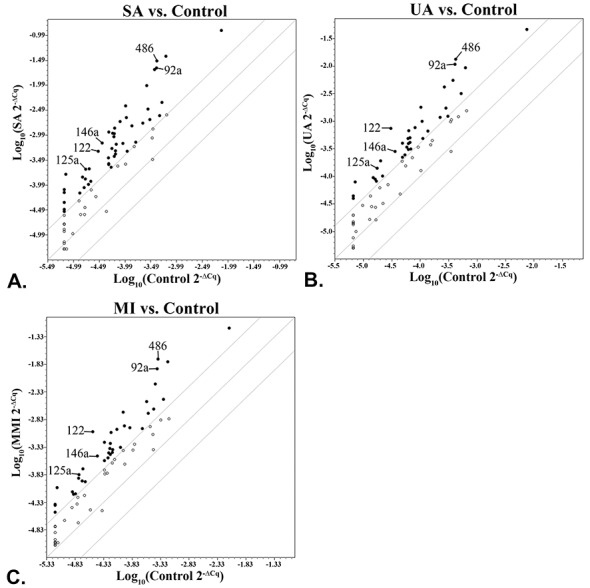
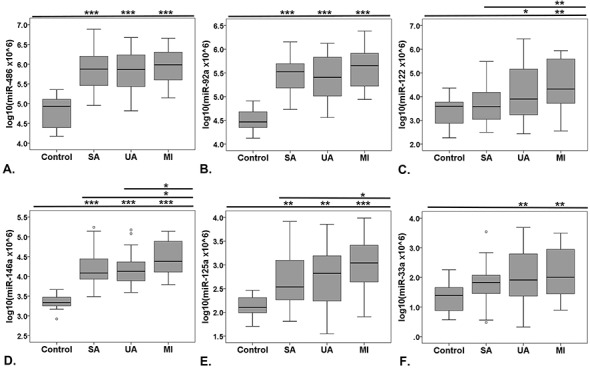
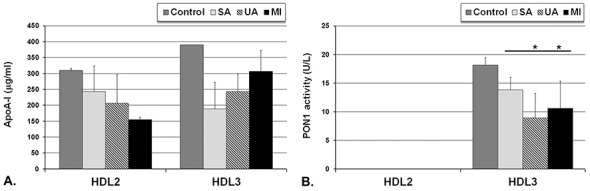
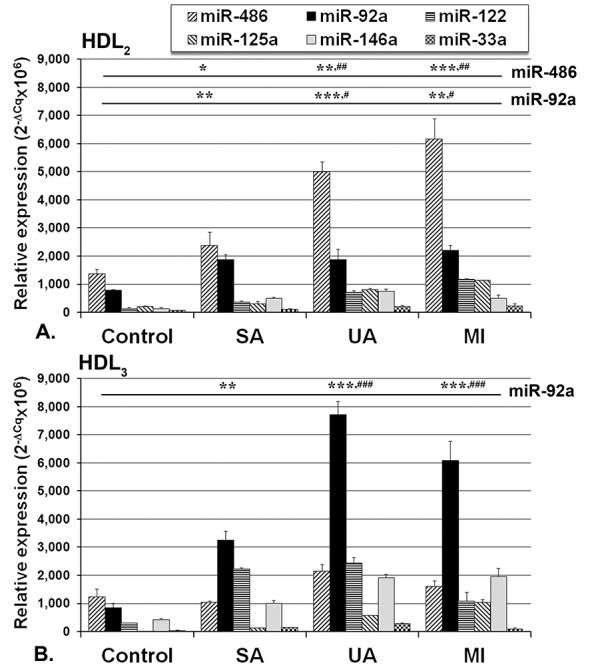
Small non-coding microRNAs (miRNAs) are implicated in gene regulation, including those involved in coronary artery disease (CAD). Our aim was to identify whether specific serum miRNAs present in the circulating lipoproteins (Lp) are associated with stable or vulnerable CAD patients. A cardiovascular disease-focused screening array was used to assess miRNAs distribution in sera collected from 95 CAD patients: 30 with stable angina (SA), 39 with unstable angina (UA), 26 at one month after myocardial infarction (MI) and 16 healthy control subjects. We found that miR-486, miR-92a and miR-122 presented the highest expression in CAD sera. These miRNA together with miR-125a, miR-146a and miR-33a were further individually analyzed by TaqMan assays. The results were consistent with PCR-array screening data that all of these miRNAs were significantly increased in CAD patients compared to controls. Using a binary logistic regression model, we established that miR-486 and miR-92a in association with some high-density lipoprotein (HDL) components can designate vulnerable CAD patients. Further, all classes of Lp were isolated from sera by density gradient ultracentrifugation. Analysis of the selected miRNAs in each Lp class showed that they were associated mainly with HDL, miR-486 and miR-92a having the highest levels. In UA and MI patients, miR-486 prevailed in HDL2, while miR-92a prevailed in HDL3, and their levels discriminate between stable and vulnerable CAD patients. We identified two circulating miRNAs that in association with some lipid metabolism biomarkers can be used as an additional tool to designate vulnerable CAD patients.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
