

Is adjuvant chemotherapy indicated in ovarian immature teratomas? A combined data analysis from the Malignant Germ Cell Tumor International Collaborative
- PMID: 26485622
- PMCID: PMC5134834
- DOI: 10.1002/cncr.29732
Is adjuvant chemotherapy indicated in ovarian immature teratomas? A combined data analysis from the Malignant Germ Cell Tumor International Collaborative
Erratum in
-
Erratum: Pashankar F, Hale JP, Dang H, et al. Is adjuvant chemotherapy indicated in ovarian immature teratomas? A combined data analysis from the Malignant Germ Cell Tumor International Collaborative. Cancer. 2016;122:230-237.Cancer. 2018 Mar 15;124(6):1302. doi: 10.1002/cncr.31266. Epub 2018 Jan 23. Cancer. 2018. PMID: 29509324 No abstract available.
Abstract
Background: There is a debate regarding the management of ovarian immature teratomas (ITs). In adult women, postoperative chemotherapy is standard except for stage I, grade 1 disease, whereas surgery alone is standard in pediatric patients. To determine the role of chemotherapy, a pooled analysis of pediatric and adult clinical trials was conducted.
Methods: Data from 7 pediatric trials and 2 adult trials were merged in the Malignant Germ Cell International Collaborative data set. Four trials included patients with newly diagnosed pure ovarian ITs and were selected (Pediatric Oncology Group/Children's Cancer Group Intergroup Study (INT 0106), Second UKCCSG Germ Cell Tumor Study (GC2), Gynecologic Oncology Group (GOG 0078 and GOG 0090). Adult and pediatric trials were analyzed separately. The primary outcome measures were event-free survival (EFS) and overall survival (OS).
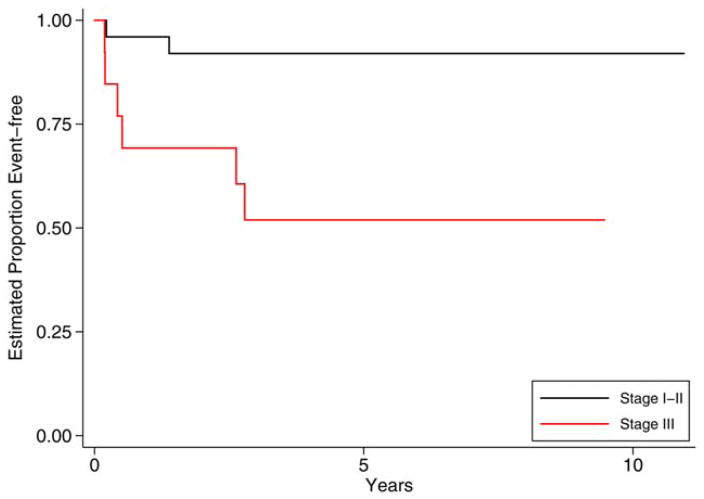
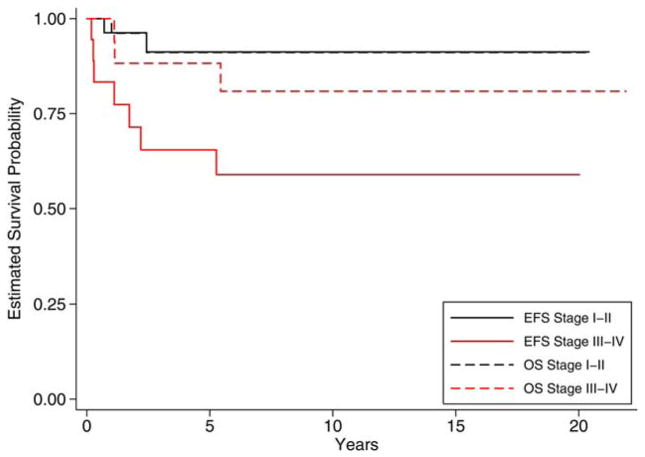
Results: One hundred seventy-nine patients were included (98 pediatric patients and 81 adult patients). Ninety pediatric patients were treated with surgery alone, whereas all adult patients received chemotherapy. The 5-year EFS and OS were 91% and 99%, respectively, for the pediatric cohort and 87% and 93%, respectively, for the adults. There were no relapses in grade 1 patients, regardless of the stage or age. Only 1 adult patient with a grade 2 IT relapsed. Among grade 3 patients, the 5-year EFS was 0.92 (0.72-0.98) for stage I/II and 0.52 (0.22-0.75) for stage III in the pediatric cohort (P = .005) and 0.91 (0.69-0.98) for stage I/II and 0.65 (0.39-0.83) for stage III/IV in the adult cohort (P = .01). Postoperative chemotherapy did not decrease relapses in the pediatric cohort.
Conclusions: The grade was the most important risk factor for relapse in ovarian ITs. Among grade 3 patients, the stage was significantly associated with relapse. Adjuvant chemotherapy did not decrease relapses in the pediatric cohort; its role in adults remains unresolved. Cancer 2016;122:230-237. © 2015 American Cancer Society.
Keywords: adult; chemotherapy; ovarian immature teratoma; pediatric.
© 2015 American Cancer Society.
Conflict of interest statement
DISCLOSURES The authors made no disclosures.
Figures
Comment in
-
Germ cell tumors: Treatment consensus across all age groups through MaGIC [Malignant Germ Cell International Collaborative].Cancer. 2016 Jan 15;122(2):181-3. doi: 10.1002/cncr.29729. Epub 2015 Oct 20. Cancer. 2016. PMID: 26485495 No abstract available.
Similar articles
-
Role of staging surgery and adjuvant chemotherapy in adult patients with apparent stage I pure immature ovarian teratoma after fertility-sparing surgery.Int J Gynecol Cancer. 2020 May;30(5):664-669. doi: 10.1136/ijgc-2019-001116. Epub 2020 Mar 15. Int J Gynecol Cancer. 2020. PMID: 32179695
-
Adjuvant chemotherapy does not improve outcome in children with ovarian immature teratoma: A comparative analysis of clinical trial data from the Malignant Germ Cell International Consortium.Pediatr Blood Cancer. 2023 Aug;70(8):e30426. doi: 10.1002/pbc.30426. Epub 2023 May 26. Pediatr Blood Cancer. 2023. PMID: 37243320
-
Surgical resection alone is effective treatment for ovarian immature teratoma in children and adolescents: a report of the pediatric oncology group and the children's cancer group.Am J Obstet Gynecol. 1999 Aug;181(2):353-8. doi: 10.1016/s0002-9378(99)70561-2. Am J Obstet Gynecol. 1999. PMID: 10454682 Clinical Trial.
-
Management of malignant ovarian immature teratoma. Role of adriamycin.Cancer. 1990 Sep 1;66(5):882-6. doi: 10.1002/1097-0142(19900901)66:5<882::aid-cncr2820660512>3.0.co;2-8. Cancer. 1990. PMID: 2201432 Review.
-
Immature Ovarian Teratoma: When to Give Adjuvant Therapy?J Pediatr Hematol Oncol. 2017 Oct;39(7):487-489. doi: 10.1097/MPH.0000000000000950. J Pediatr Hematol Oncol. 2017. PMID: 28859031 Review.
Cited by
-
Outcome of patients with stage I immature teratoma after surveillance or adjuvant chemotherapy.Front Oncol. 2024 Feb 2;14:1330481. doi: 10.3389/fonc.2024.1330481. eCollection 2024. Front Oncol. 2024. PMID: 38371620 Free PMC article.
-
Ovarian teratoma in children: a plea for collaborative clinical study.J Ovarian Res. 2018 Aug 30;11(1):75. doi: 10.1186/s13048-018-0448-2. J Ovarian Res. 2018. PMID: 30165903 Free PMC article.
-
Ovarian cystectomy in the treatment of apparent early-stage immature teratoma.J Int Med Res. 2017 Apr;45(2):771-780. doi: 10.1177/0300060517692149. Epub 2017 Jan 1. J Int Med Res. 2017. PMID: 28415950 Free PMC article.
-
What recent primary studies tell us about ovarian teratomas in children: a scoping review.Cancer Metastasis Rev. 2020 Mar;39(1):321-329. doi: 10.1007/s10555-020-09844-3. Cancer Metastasis Rev. 2020. PMID: 32006216 Free PMC article.
-
A case series and literature review on 98 pediatric patients of germ cell tumor developing growing teratoma syndrome.Cancer Med. 2023 Jun;12(12):13256-13269. doi: 10.1002/cam4.6017. Epub 2023 May 4. Cancer Med. 2023. PMID: 37140211 Free PMC article. Review.
References
-
- Gobel U, Calaminus G, Blohm M, et al. Extracranial non-testicular teratoma in childhood and adolescence: introduction of a risk score for stratification of therapy. Klin Padiatr. 1997;209:228–234. - PubMed
-
- Heifetz SA, Cushing B, Giller R, et al. Immature teratomas in children: pathologic considerations. Am J Surg Pathol. 1998;22:1115–1124. - PubMed
-
- Norris HJ, Zirkin HJ, Benson WL. Immature (malignant) teratoma of the ovary: a clinical and pathologic study of 58 cases. Cancer. 1976;37:2359–2372. - PubMed
-
- Gershenson DM, del Junco G, Silva EG, Copeland LJ, Wharton JT, Rutledge FN. Immature teratoma of ovary. Obstet Gynecol. 1986;68:624–629. - PubMed
-
- Cushing B, Giller R, Ablin A, et al. Surgical resection alone is effective treatment for ovarian immature teratoma in children and adolescents: a report of the Pediatric Oncology Group and the Children’s Cancer Group. Am J Obstet Gynecol. 1999;181:353–358. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
