

Adolescents with or at ultra-high risk for bipolar disorder exhibit erythrocyte docosahexaenoic acid and eicosapentaenoic acid deficits: a candidate prodromal risk biomarker
- PMID: 26486098
- PMCID: PMC4818707
- DOI: 10.1111/eip.12282
Adolescents with or at ultra-high risk for bipolar disorder exhibit erythrocyte docosahexaenoic acid and eicosapentaenoic acid deficits: a candidate prodromal risk biomarker
Abstract
Aim: Mood disorders are associated with low levels of the long-chain omega-3 (LCn-3) fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). This study investigated LCn-3 fatty acid biostatus in youth with or at varying risk for developing mania to assess its utility as a prodromal risk biomarker.
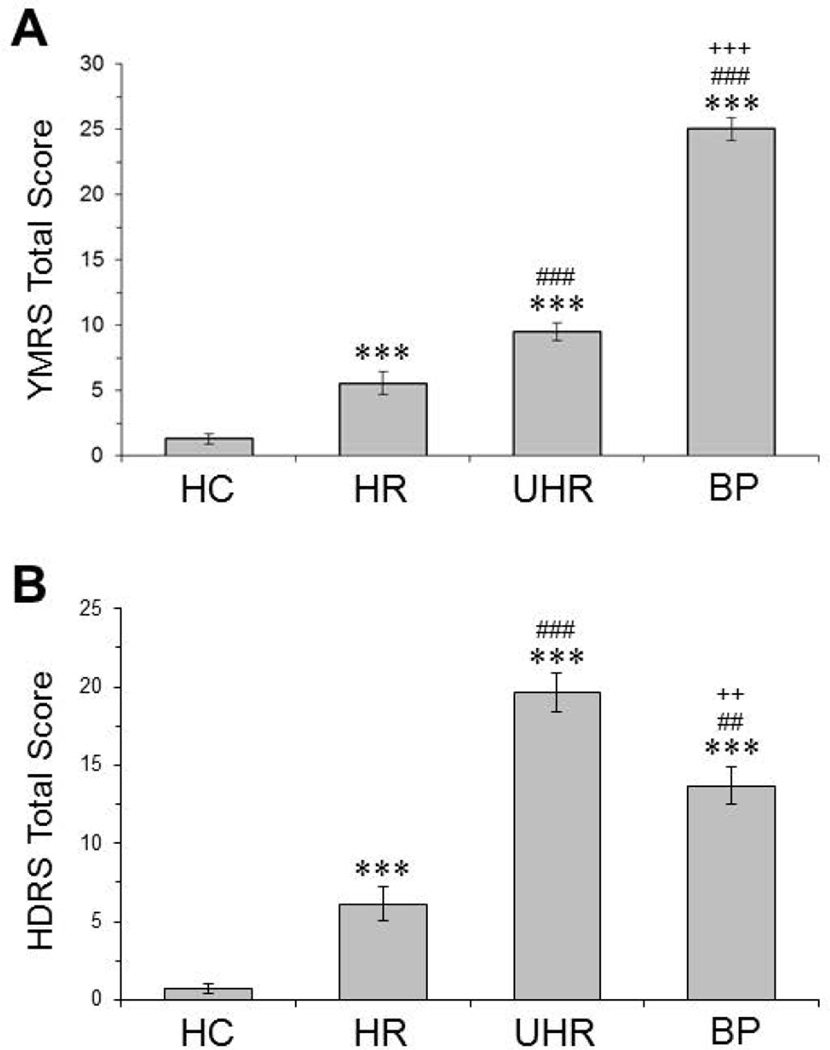
Method: Erythrocyte fatty acid composition was determined in healthy adolescents (n = 28, HC), asymptomatic adolescents with a biological parent with bipolar I disorder (n = 30; 'high risk', HR), adolescents with a biological parent with bipolar I disorder and major depressive disorder, or depressive disorder not otherwise specified (n = 36; 'ultra-high risk', UHR), and first-episode adolescent bipolar manic patients (n = 35, BP).
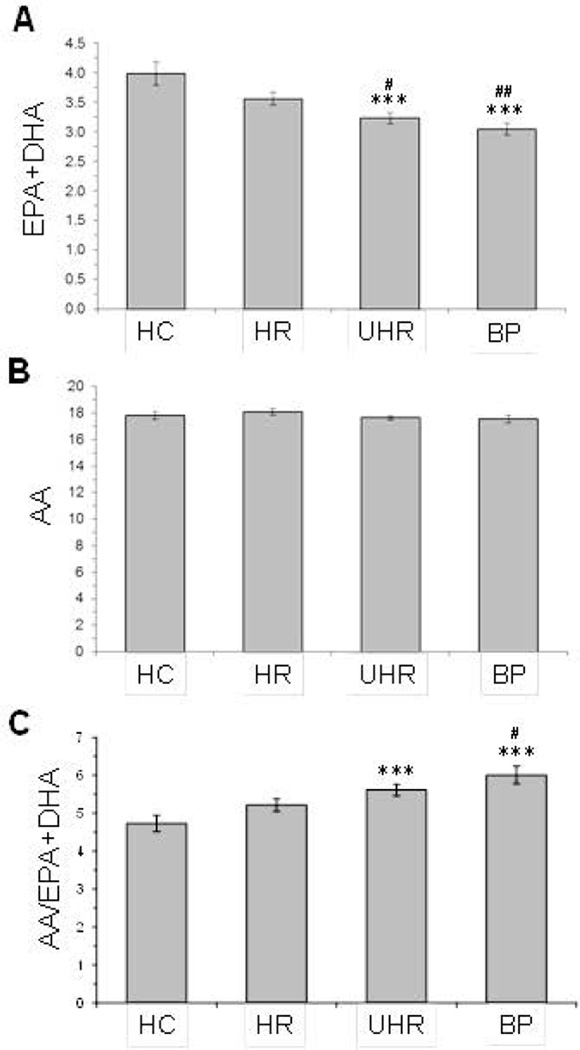
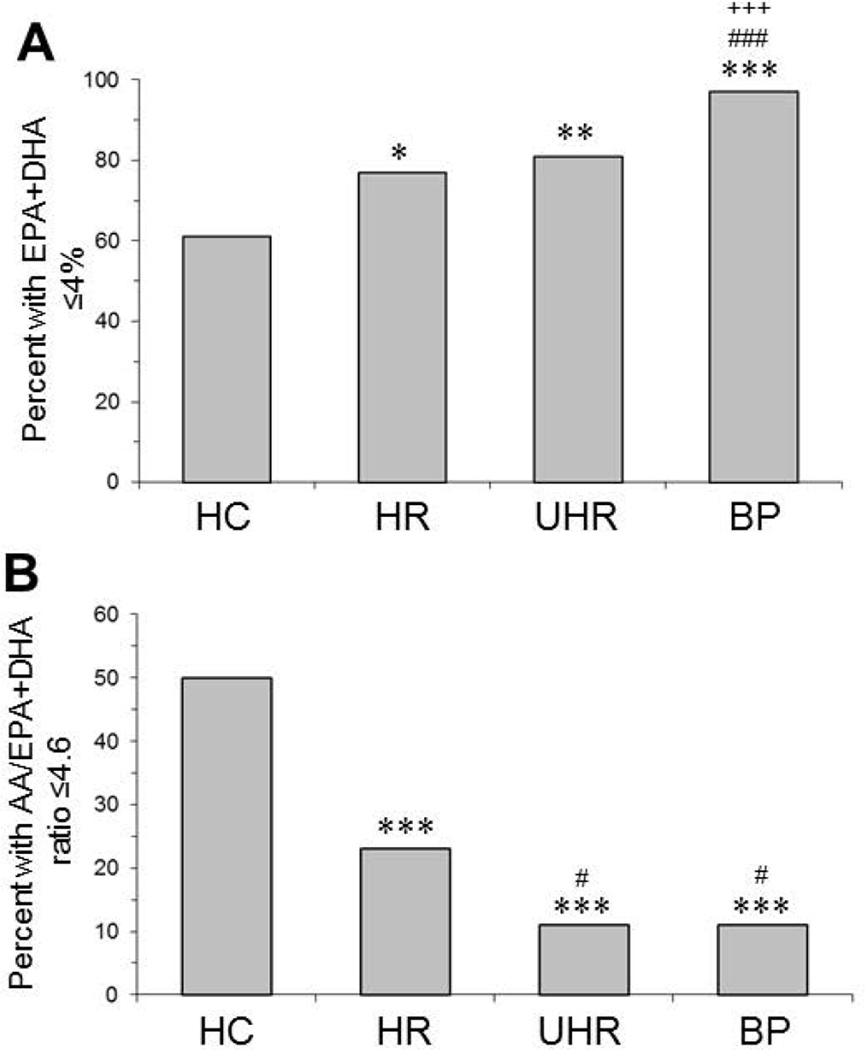
Results: Group differences were observed for DHA (P ≤ 0.0001) and EPA (P = 0.03). Compared with HC, erythrocyte EPA + DHA ('omega-3 index') was significantly lower in BP (-24%, P ≤ 0.0001) and UHR (-19%, P = 0.0006) groups, and there was a trend in the HR group (-11%, P = 0.06). Compared with HC (61%), a greater percentage of HR (77%, P = 0.02), UHR (80%, P = 0.005) and BP (97%, P = 0.001) subjects exhibited EPA + DHA levels of ≤4.0%. Among all subjects (n = 130), EPA + DHA was inversely correlated with manic (r = -0.29, P = 0.0008) and depressive (r = -0.28, P = 0.003) symptom severity. The AA/EPA + DHA ratio was significantly greater in BP (+22%, P = 0.0002) and UHR (+16%, P = 0.001) groups.
Conclusions: Low EPA + DHA levels coincide with the initial onset of mania, and increasing risk for developing bipolar disorder is associated with graded erythrocyte EPA + DHA deficits. Low erythrocyte EPA + DHA biostatus may represent a promising prodromal risk biomarker warranting additional evaluation in future prospective studies.
Keywords: arachidonic acid (AA); eicosapentaenoic acid (EPA); mania; omega-3 index; ultra-high risk.
© 2015 Wiley Publishing Asia Pty Ltd.
Figures
Comment in
-
Could erythrocyte omega-3 fatty acid levels be harbingers of bipolar disorder?Early Interv Psychiatry. 2016 Jun;10(3):191-2. doi: 10.1111/eip.12320. Early Interv Psychiatry. 2016. PMID: 27037962 No abstract available.
Similar articles
-
Familial risk for bipolar I disorder is associated with erythrocyte omega-3 polyunsaturated fatty acid deficits in youth with attention-deficit hyperactivity disorder.Psychiatry Res. 2022 Jul;313:114587. doi: 10.1016/j.psychres.2022.114587. Epub 2022 May 4. Psychiatry Res. 2022. PMID: 35550258
-
First-episode bipolar disorder is associated with erythrocyte membrane docosahexaenoic acid deficits: Dissociation from clinical response to lithium or quetiapine.Psychiatry Res. 2015 Dec 15;230(2):447-53. doi: 10.1016/j.psychres.2015.09.035. Epub 2015 Oct 9. Psychiatry Res. 2015. PMID: 26477955 Free PMC article.
-
Meta-analysis of erythrocyte polyunsaturated fatty acid biostatus in bipolar disorder.Bipolar Disord. 2016 May;18(3):300-6. doi: 10.1111/bdi.12386. Epub 2016 Apr 18. Bipolar Disord. 2016. PMID: 27087497 Free PMC article.
-
Detection and treatment of omega-3 fatty acid deficiency in psychiatric practice: Rationale and implementation.Lipids Health Dis. 2016 Feb 10;15:25. doi: 10.1186/s12944-016-0196-5. Lipids Health Dis. 2016. PMID: 26860589 Free PMC article. Review.
-
Evaluation of docosahexaenoic acid deficiency as a preventable risk factor for recurrent affective disorders: current status, future directions, and dietary recommendations.Prostaglandins Leukot Essent Fatty Acids. 2009 Aug-Sep;81(2-3):223-31. doi: 10.1016/j.plefa.2009.05.017. Epub 2009 Jun 9. Prostaglandins Leukot Essent Fatty Acids. 2009. PMID: 19515544 Review.
Cited by
-
Microalgae n-3 PUFAs Production and Use in Food and Feed Industries.Mar Drugs. 2021 Feb 18;19(2):113. doi: 10.3390/md19020113. Mar Drugs. 2021. PMID: 33670628 Free PMC article. Review.
-
Effect of non-invasive spinal cord stimulation in unmedicated adults with major depressive disorder: a pilot randomized controlled trial and induced current flow pattern.Mol Psychiatry. 2024 Mar;29(3):580-589. doi: 10.1038/s41380-023-02349-9. Epub 2023 Dec 20. Mol Psychiatry. 2024. PMID: 38123726 Free PMC article. Clinical Trial.
-
Perinatal dietary omega-3 fatty acid deficiency reduces maternal nurturing behavior in rats: dissociation from elevated pro-inflammatory signaling.Nutr Neurosci. 2021 Sep;24(9):735-746. doi: 10.1080/1028415X.2019.1674507. Epub 2019 Oct 10. Nutr Neurosci. 2021. PMID: 31599208 Free PMC article.
-
Nutraceuticals in Psychiatric Disorders: A Systematic Review.Int J Mol Sci. 2024 Apr 28;25(9):4824. doi: 10.3390/ijms25094824. Int J Mol Sci. 2024. PMID: 38732043 Free PMC article.
-
Lipid Biomarker Research in Bipolar Disorder: A Scoping Review of Trends, Challenges, and Future Directions.Biol Psychiatry Glob Open Sci. 2023 Jul 23;3(4):594-604. doi: 10.1016/j.bpsgos.2023.07.004. eCollection 2023 Oct. Biol Psychiatry Glob Open Sci. 2023. PMID: 37881590 Free PMC article.
References
-
- Perlis RH, Miyahara S, Marangell LB, Wisniewski SR, Ostacher M, DelBello MP, Bowden CL, Sachs GS, Nierenberg AA. STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the systematic treatment enhancement program for bipolar disorder (STEP-BD) Biol Psychiatry. 2004;55:875–881. - PubMed
-
- Perlis RH, Dennehy EB, Miklowitz DJ, Delbello MP, Ostacher M, Calabrese JR, Ametrano RM, Wisniewski SR, Bowden CL, Thase ME, Nierenberg AA, Sachs G. Retrospective age at onset of bipolar disorder and outcome during two-year follow-up: results from the STEP-BD study. Bipolar Disord. 2009;11:391–400. - PMC - PubMed
-
- Smoller JW, Finn CT. Family, twin, and adoption studies of bipolar disorder. Am J Med Genet C Semin Med Genet. 2003;123C:48–58. - PubMed
-
- DelBello MP, Geller B. Review of studies of child and adolescent offspring of bipolar parents. Bipolar Disord. 2001;3:325–334. - PubMed
-
- Goodwin FK, Jamison KR. Manic-Depressive Illness: Bipolar Disorders and Recurrent Depression. 2nd Edition. New York: Oxford University Press; 2007.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
